![[NASA Logo]](../Images/nasaball.gif)
| |
NASA Procedures and Guidelines |
This Document is Obsolete and Is No Longer Used.
|
|
P.1 Purpose
P.2 Applicability
P.3 Authority
P.4 Applicable Documents and Forms
P.5 Measurement/Verification
P.6 Cancellation
1.1 Designated Agency Safety and Health Official
1.2 Medical Waiver Authority
1.3 General Center Responsibilities
1.4 Required Annual Reports
1.5 Drug-Free Workplace
1.6 Credentialing, Education, and Training of Occupational Health Professionals
1.7 Web Site Initiatives and Capabilities
1.8 Support of Federal and Interagency Initiatives
1.9 Occupational Health Program Periodic Review Overview
1.10 Recordkeeping, General
2.1 Occupational Medicine, General
2.2 Medical Quality Assurance
2.3 Disease and Injury Prevention
2.4 Diagnosis and Treatment of Occupational Illness or Injury
2.5 Immunizations
2.6 Medical Support to Emergency Preparedness Planning
2.7 Pandemic Planning
2.8 Physical Examinations
2.9 Emergency Medical Services
2.10 Automated External Defibrillator (AED) Program
2.11 Bloodborne Pathogens
2.12 Infection Control
2.13 Medical Record Management
2.14 Shift Work and Balancing Work-Rest Cycles
2.15 International Travel or Assignment
3.1 Primary Prevention and Health Promotion
3.2 Primary Prevention
3.3 Fitness Centers
4.1 General
4.2 Occupational Exposure Limits (OEL's)
4.3 Occupational Exposure Assessment and Management
4.4 Sampling, Analytical Methods, and Equipment Calibration
4.5 Reproductive and Developmental Health
4.6 Nanotoxicology
4.7 Control of Hazardous Substances and Articles Acquisitions
4.8 Hearing Conservation
4.9 Ergonomics
4.10 Indoor Air Quality
4.11 Biosafety
4.12 Food Safety
4.13 Radiation, General
4.14 Radioactive Materials
4.15 Ionizing Radiation-Generating Equipment
4.16 Laser and Non-laser Optical Radiation
4.17 Radio Frequency Electromagnetic Radiation
5.1 General
5.2 EAP Confidentiality
5.3 EAP Record Access
5.4 Release of Case Information and Secondary Disclosure
5.5 EAP Roles
5.6 Responsibilities
5.7 Program Elements
6.1 General
6.2 Presidential Orders and Department of Labor Initiatives
6.3 Chargeback
6.4 Roles
6.5 Responsibilities
6.6 Employee Eligibility to File a Claim
6.7 Employee Requirement to File Claim
6.8 Determining Compensability of a Claim
6.9 Records and Confidentiality
6.10 Recordkeeping, Retention, and Requests for Copies
6.11 Federal Workers' Compensation • General Process
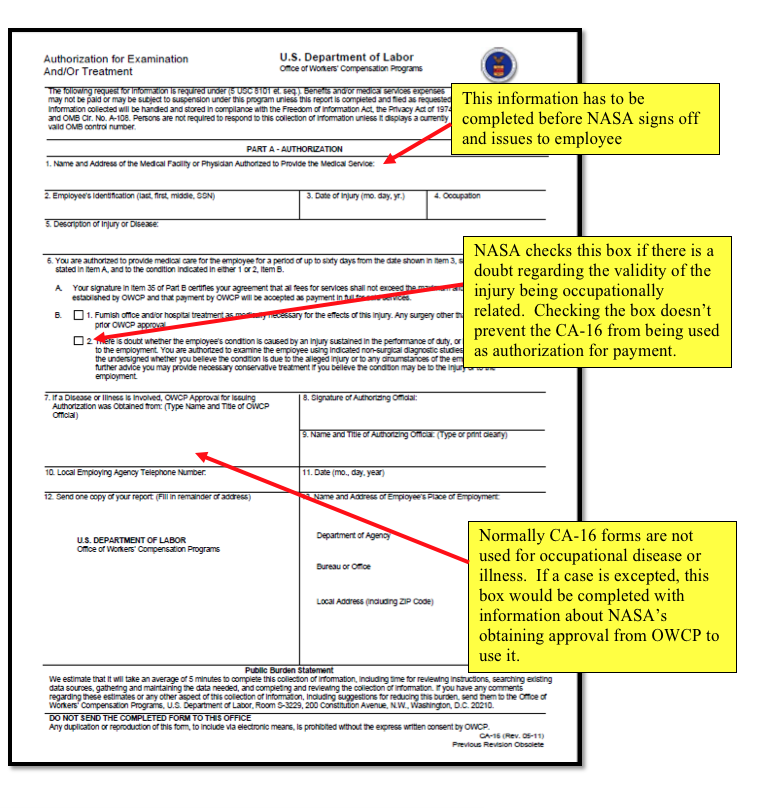
6.12 Traumatic Injury Claims: Form CA-16, Continuation of Pay, and Controversion
6.13 Occupational Disease/Exposure/Illness
6.14 Employee Appeals for Denial of Claim
7.1 Policy
7.2 Agency and Center Occupational Health Reviews
7.3 Agency Occupational Health Periodic Reviews
7.4 Responsibilities
7.5 Agency Occupational Health Review Process Description
7.6 Center Self-Reviews
|
|
|
|
|
1 |
10/02/2018 |
Updated Appendix C., with administrative changes |
|
2 |
04/03/2019 |
Administrative changes made to 1) include additional applicable documents to section P.4; 2) clarify requirement in paragraph 4.12.1.4; 3) update definitions in Appendix B; 4) update Appendix C; and 5) clarify employee rights to file claims if injured while working from home in paragraph 6.11.2.1. |
|
3 |
09/11/2019 |
Updated Chapter 4, with requirements for Farmers Markets included in para 4.12 and definitions for the following were included in Appendix A: Cottage Foods; Cottage Food Vendor; Farmers Market; Farmers Market Vendor; Food Safety Inspectors; Market Manager; Produce; and Time/Temperature Control for Safety Food. |
a. This NASA Procedural Requirement (NPR) describes Occupational Health Program (OHP) procedures necessary to effectively carry out the mission of the Office of the Chief Health and Medical Officer (OCHMO) and ensure that the scope and quality of services provided by the OHP personnel at Centers are optimal. OHP professionals and allied health professionals throughout the Agency shall utilize these procedures in their daily tasks to ensure the health of employees and a safe work environment.
b. Where conflicts exist between other NASA health and safety requirements, Occupational Safety and Health Administration requirements and other Federal, state, or local regulations, the most protective requirements shall apply. The NASA Chief Health and Medical Officer (CHMO) is the final authority on the applicability of all Occupational Health (OH) requirements throughout the Agency.
c. OHP services encompass five constituent areas, as a holistic approach; all working synergistically to support employee health, yet functioning under different legal statutes and requiring unique professional expertise and different process procedures and outcome metrics. These five constituent programs include Occupational Medicine, Environmental Health (including Radiological Health), Health Promotion and Wellness, Federal Workers' Compensation, and Employee Assistance.
d. Recordkeeping is one area that overlaps all OHP constituent areas. While each area has recordkeeping requirements specific to it, there are a few requirements that apply across the board. All OHP records shall be safeguarded, maintained, and dispositioned 1 in accordance with the following:
(1) NPR 1441.1, NASA Management Program Requirements;
(2) NRRS 1441.1, NASA Record Retention Schedules;
(3) Privacy Act of 1974, as amended, 5 U.S.C. 552a;
(4) The Health Information Management System (HIMS) in NASA's "Privacy Act; Annual Notice and Amendment to Systems of Records," published in the Federal Register;
(5) Records Management Plan for the NASA Electronic Health Record System, NASA-EHRS-RMP-000, February 28, 2012; and
(6) Genetic Information Nondiscrimination Act of 2008 (GINA), PL 110-233.
a. This NPR is applicable to NASA Headquarters (HQ) and NASA Centers, including Component Facilities and Technical and Service Support Centers. This language applies to the Jet Propulsion Laboratory (JPL), other contractors, grant recipients, or parties to agreements only to the extent specified or referenced in the appropriate contracts, grants, or agreements. Portions of this NPR are applicable to visitors.
b. The OCHMO is a staff office that issues policy and provides guidance, Center technical support, and periodic reviews of Centers' OH programs. Periodic reviews shall not be considered direct "oversight" of Center programs and/or processes. Oversight, and implementation of policies set herein, is the responsibility of NASA Centers, Component Facilities, Service Support Centers, other NASA installations, and the NASA Management Office at the JPL (hereafter called "Centers").
c. The section of this NPR requiring the mandatory use of an electronic health record system (EHRS) does not apply to JPL.
d. In this NPR "shall" denotes a mandatory requirement, "may" or "can" denotes a discretionary privilege or permission, "should" denotes a good practice, and "will" denotes an expected outcome.
a. Health Services Programs, 5 U.S.C. § 7901.
b. The Occupational Safety and Health Act of 1970, as amended, 29 U.S.C. § 668, Section 19.
c. The National Aeronautics and Space Act, as amended, 51 U.S.C. § 20113.
d. Basic Program Elements for Federal Employee Occupational Safety and Health Programs and Related Matters, 29 CFR pt. 1960.
e. Occupational Safety and Health Programs for Federal Employees, E.O. 12196 (1980), dated February 26, 1980.
a. Federal Employees' Compensation Act, 5 U.S.C. § 8101, et seq.
b. Physical qualification standards for an individual with diabetes mellitus treated with insulin for control, 49 CFR pt. 46.
c. Physical Qualifications and Examinations, 49 CFR subpt. E.
d. NPD 1000.0, Strategic Management and Governance Handbook.
e. NPD 1210.2, NASA Surveys, Audits, and Reviews Policy.
f. NPD 1600.3, Policy on Prevention of and Response to Workplace Violence.
g. NPD 1850.1, NASA Medical System Quality Assurance.
h. NPR 1000.3, The NASA Organization.
i. NPR 1850.1, Quality Assurance of the NASA Medical Care System.
j. NASA Laser Safety Review Board (LSRB) Charter, April 2014.
k. Department of Federal Employees' Compensation Procedure Manual.
The triennial review process and interim Center self-reviews are used to measure program performance.
NPR 1800.1C, NASA Occupational Health Program Procedures, dated October 6, 2009.
/s/
Richard S. Williams
1.1.1 The Chief Health and Medical Officer (CHMO) is the Designated Agency Safety and Health Officer (DASHO) and liaison to the Department of Labor (DOL).
1.1.2 All official, Agency-related communication with the Occupational Safety and Health Administration (OSHA) shall be through the DASHO.
1.1.3 The Center/Facility Director shall notify the DASHO within one hour when OSHA, Nuclear Regulatory Commission (NRC), or other occupational safety or health regulatory inspectors arrive on a NASA Center or Facility for the purpose of conducting an inspection or visit as per NPR 8715.1.
1.2.1 As described in NPR 7120.11, the CHMO is the Agency Health and Medical Technical Authority (HMTA) for all health and medical technical requirements, standards, and matters. The CHMO possesses the final waiver authority for any NASA health and medical requirement and is the final interpretation authority on the applicability of all occupational health requirements across the Agency.
1.2.2 The CHMO gives medical authority to each Center's Chief Health Officer/Medical Director.
1.2.3 The CHMO promotes the health and safety of Agency personnel in space and on the ground. The CHMO develops medical policy, establishes guidelines for health and medical practice, provides guidance for health care delivery, promotes professional competency, and reviews/approves human and animal research requirements across the Agency.
1.2.4 The CHMO serves as the HMTA for NASA-unique occupational health requirements included in:
a. Section 2.15, Shift Work and Balancing Work-Rest Cycles.
b. Section 4.2, Occupational Exposure Limits (OELs).
c. Section 4.5, Reproductive and Developmental Health.
d. Section 4.6, Nanotoxicology.
e. Section 4.8, Hearing Conservation.
1.3.1 Centers shall advocate for budget and resources for occupational health programs to ensure compliance with OSHA, state, and local standards and NASA requirements. If a reduction in budget is anticipated to have a significant impact on the delivery of Occupational Health (OH) services, the OCHMO shall be immediately informed.
1.3.2 Center occupational health practitioners (e.g., physicians, nurses, industrial hygienists, health physicists, physical fitness professionals) shall be familiar with employees' tasks and work environment to better understand specific OH issues and cases, as well as the mechanism of injury, exposure, or illness; and evaluate safety and OH concerns.
1.3.3 Agency and Center Purchase Requesters/Requirements Initiators shall coordinate with Center OH offices to ensure requirements documents include all pertinent OH requirements.
1.3.4 Agency and Center Procurement organizations shall work with Center OH offices and Purchase Requesters/Requirements Initiators to ensure that all pertinent OH Federal and Agency provisions/clauses are included in contracts.
1.3.5 Centers shall ensure that all pertinent OH requirements are included in commercial partners, Space Act Agreements, other Federal agencies, international parties, and tenant agreements.
1.3.6 Centers shall implement effective OH programs as measured by the Agency's triennial OH review program.
1.4.1 OSHA Report
1.4.1.1 NASA submits an annual report to the Secretary of Labor containing the status of NASA's Safety and Health Programs during the preceding year, goals and objectives for the current year, and a plan for achieving those goals. The procedure for collecting the requisite data is as follows:
a. The NASA Office of the Chief Health and Medical Officer (OCHMO) and the Office of Safety and Mission Assurance (OSMA) electronically forward the OSHA Annual Report format to the Centers each year soon after it is received from OSHA with a prescribed deadline for submission of the OSHA-requested information to the OCHMO.
b. The Safety and Health organizations at NASA Centers jointly complete the form, provide the associated documentation, and return all OSHA requested information to the OCHMO and the OSMA in the prescribed format and electronic media by the designated deadline.
c. Other NASA organizations shall support information compilation, editing, and writing of the OSHA Annual Report effort as needed.
d. The report shall be jointly prepared by the OCHMO and the OSMA, jointly signed by the DASHO and the Director, Safety and Assurance Requirements Division, and submitted to OSHA.
1.5.1.1 The overall responsibility for NASA's Drug-Free Workplace Program (DFWP) lies with the Office of the Chief Human Capital Officer (OCHCO), with policies and procedures provided in NPR 3792.1. The OCHMO supports DFWP by ensuring Employee Assistance Programs (EAPs) across the Agency support the requirements of the program. The Agency Medical Review Officer assigned to all Centers is located at the NASA Shared Services Center.
1.5.1.2 The OCHMO supports the DFWP through management of NASA Center EAP policy.
1.6.1 General
1.6.1.1 All Occupational Health (OH) professional disciplines (Occupational Medicine (OM), Industrial Hygiene (IH), Health Physics (HP), Food Sanitation (FS), EAP, Federal Workers' Compensation (FWC), and Fitness) shall comply at all times with Federal, state, and professional requirements applicable to their respective disciplines.
1.6.2 Responsibilities
1.6.2.1 Credentialing and privileging of all licensed medical practitioners and non-licensed health-care support personnel providing health care for Agency personnel shall be governed by the requirements contained in NPR 1850.1, Quality Assurance of the NASA Medical Care System.
1.6.2.2 Centers shall establish and maintain effective organizations to fulfill OH requirements using professionally qualified persons, ensuring discipline-specific professional licensures, certifications, and accreditations necessary for operations are maintained.
1.6.2.3 NASA fully uses a Commercial Off-the-Shelf (COTS) Electronic Health Records System and has trained all Centers in its operation. As clinic contracts are re-negotiated and perhaps changed, it is the Center's responsibility to ensure that every clinic has a least one individual, other than the Medical Director, dedicated to operating and using the Agency's chosen electronic medical records system.
1.6.3 Process Description
1.6.3.1 Center hiring policies shall comply with Federal and NASA credentialing requirements and with state licensure statutes.
1.6.3.2 Centers shall hire OH professionals with experience and credentials commensurate with program requirements.
1.6.3.3 Centers shall have a process to ascertain and promote education, training, and credentialing requirements for all civil service and contractor OH program personnel that is commensurate with program needs.
1.6.3.4 Centers shall conduct assessments of OH professional and career development needs to determine the training required of their OH staff. These needs shall be communicated to Center management to meet professional OH licensure and certification.
1.7.1 General
1.7.1.1 NASA OCHMO's Web sites include the Agency OH Web site and public access Web site which shall be available as resources for dissemination of OH related information to OH personnel to assist OCHMO in communicating to the Centers.
1.7.2 Responsibilities
1.7.2.1 The OCHMO maintains the Agency OH Web site as a means of disseminating information and providing guidance to NASA Centers and Facilities on OH-related topics and policies.
1.7.2.2 Centers shall refer to the Agency OH Web site for recommendations on meeting program requirements. NASA OH Documents, Guidelines, and Checklists referenced on the Agency OH Web site.
1.7.3 Process Description
1.7.3.1 The Agency OH Web site content meets all of NASA's security, accessibility, and data privacy regulations.
1.7.3.2 The Agency OH Web site shall be designed to meet the various NASA OH community needs.
1.8.1 General
1.8.1.1 The OCHMO collaborates with the Office of Personnel Management (OPM) on health and work/life policies and initiatives.
1.8.1.2 The OCHMO provides guidance to Center Contracting Officer Representatives (CORs) on Center-specific health and work/life policies, and periodically reviews Center implementation of these policies.
1.8.2 Responsibilities
1.8.2.1 Centers shall adopt policies and implement programs in support of a healthy work environment as directed by the OCHMO, based on guidance from the OPM and other Federal authorities pertaining to work/life issues.
1.8.2.2 The Medical CORs and the Medical Director shall actively support all CHMO-directed health initiatives.
1.8.2.3 The Health Promotion Workgroup (HPW) Team members shall coordinate all efforts at the Center level.
1.8.3 Process Description
1.8.3.1 The CHMO communicates Agency-sanctioned work/life and health and productivity initiatives to the Centers.
1.8.3.2 The Centers implement all Agency-directed initiatives, as appropriate, to their Center populations and to the extent they are able to provide.
1.9.1 General
1.9.1.1 The review process assesses OH program efficacy at all Centers for the following disciplines:• OM, IH, HP, FS, Fitness Center (FC), and EAP.• The FWC case management for the Agency is reviewed at the Johnson Space Center (for astronaut claims) and the NASA Shared Services Center (for all other NASA claims). The review of FWC case management handled at the NASA Shared Services Center will take place whenever an onsite OH review is conducted at the Stennis Space Center.
1.9.2 Responsibilities
1.9.2.1 The OCHMO assesses the effectiveness of the Agency's OH programs at all Centers. To carry out this responsibility, it conducts periodic onsite reviews of OH programs at all Centers.
1.9.2.2 Center Directors shall be responsible for providing adequate provisions and resources in support of an Agency review. This includes providing requested documentation and information in a timely fashion and in an orderly arrangement; onsite office and meeting room accommodations; information technology support; and a status of the OH programs at in-briefings. It also includes: identifying discipline-specific points of contact (POC); being present for and supporting the onsite review activities; and responding with corrective actions to review findings in a timely manner.
1.9.3 Process Description
1.9.3.1 A detailed description of the review process is found in Chapter 7 of this document.
1.10.1 General
1.10.1.1 Centers shall ensure that all OH contracts, at the time of their negotiation, expressly require record keeping of any and all records containing personnel health information as per Center needs.
1.10.1.2 All occupational health records at the Centers are NASA records and shall be retained at the Centers regardless of contract changes and dispositioned in accordance with NASA's record requirements and this NPR.
1.10.2. Responsibility
1.10.2.1 The Center shall ensure that each new OH contract or contract renewal contain specific language on record keeping requirements.
2.1.1 General
2.1.1.1 The OM clinics shall meet all applicable requirements of Federal and state regulations, professional standards, the NASA Medical Quality Assurance (QA) Program, and other NASA program requirements.
2.1.2 Responsibilities
2.1.2.1 The CHMO shall establish policy requirements for the OM programs.
2.1.2.2 The Director of Health and Medical Systems shall ensure the oversight and advocacy of Center OM programs through regular periodic reviews.
2.1.2.3 The OCHMO shall have the opportunity to review any significant request for a change or relief of OH policy.
2.1.2.4 The Medical COR at each Center shall advocate for funding to meet all programmatic requirements within the scope of service being provided.
2.1.2.5 The Center Medical Director shall be responsible for meeting all Federal, state, and NASA requirements for that jurisdiction.
2.1.2.6 The NASA OH personnel shall notify the CHMO when a Medical Director change occurs at their Center.
2.1.3 Process Description
2.1.3.1 The NASA CHMO and Director of Health and Medical Systems shall be informed immediately of any of the following occupational health-related incidents at NASA Centers from:
a. Any employee death on duty;
b. Cluster investigations;
c. Infectious disease outbreaks;
d. Automatic External Defibrillator (AED) use and outcome;
e. Quality of care issues;
f. Workplace violence;
g. Regulatory Agency (e.g., Occupational Safety and Health Administration, Nuclear Regulatory Agency) inspection/investigation; and
h. Medical incident or evacuation of civil service employees on official Government foreign travel.
NOTE: All mishaps must be reported in accordance with NPR 8621.1, NASA Procedural Requirements for Mishap Reporting, Investigating, and Recordkeeping and the appropriate Center Mishap Preparedness and Contingency Plan.
2.1.3.2 Center OM physicians and other healthcare providers (e.g., nurse practitioners, physician assistants) shall be appropriately credentialed and privileged in compliance with the requirements of the NASA Medical QA program.
2.1.3.2.1 The OM staff shall be trained for the tasks they are required to perform and meet all regulatory and NASA training requirements.
2.1.3.3 Center CORs shall be responsible for advocating adequate budget and resources for OM clinics to provide services.
2.1.3.3.1 If a reduction in budget is anticipated to have a significant impact on the delivery of OM services, the OCHMO shall be informed.
2.2.1 General
2.2.1.1 All NASA OM clinics shall establish a medical quality assurance program that meets these requirements and all of the requirements found in NPD 1850.1, NASA Medical System Quality Assurance; NPR 1850, Quality Assurance of the NASA Medical Care System; and the NASA Medical QA Program Desk Guide found on the Agency OH Web site.
2.2.2 Responsibilities
2.2.2.1 The CHMO shall set medical quality assurance program policy.
2.2.2.2 The Director of Health and Medical Systems shall ensure compliance with OH medical QA policy through regular periodic reviews.
2.2.2.3 The COR is responsible for advocating for sufficient resources to implement a medical quality assurance program.
2.2.2.4 The Center's medical staff is responsible for developing the Center policies and procedures and implementing a medical QA program.
2.2.3 Process Description
2.2.3.1 A comprehensive set of policies and procedures shall be developed to meet the quality of care standards.
2.2.3.1.1 The policies and procedures shall meet all the requirements of the Employee-Directed Principles (Managing Employee Assessment, Employee Care Process, Coordinating Employee Care, Employee Care Rights, and Employee Healthcare Education) and Management-Directed Principles (Facility and Safety Management, Governance, Information Management Services, Infection Control Services, Performance Improvement Management, and Staff Qualifications and Competency) as found on the Agency OH Web site.
2.2.3.2 The OM clinics shall establish and monitor medical QA program metrics to evaluate the program effectiveness.
2.3.1 General
2.3.1.1 NASA OH programs shall encompass primary prevention, health promotion, and a comprehensive safety program that impacts both individual health and Agency wellness.
2.3.2 Responsibilities
2.3.2.1 Center Occupational Health Program (OHP) personnel shall provide a variety of prevention services such as medical examinations, health and wellness promotions, immunizations, food safety and sanitization services, assorted health screenings, and control of chemical and physical hazards.
2.3.3 Process Description
2.3.3.1 Health Promotion Programs shall be implemented through both Agency-directed and Center-planned activities.
2.3.3.2 The efficacy of primary prevention activities shall be documented with appropriately selected metrics for benchmarking, continuous improvement of programs, and resource allocation.
2.4.1 General
2.4.1.1 NASA Centers shall ensure timely diagnosis and treatment of occupational injuries and illnesses and act to minimize the recurrence of a similar problem in other coworkers and those in similar jobs.
2.4.2 Responsibilities
2.4.2.1 The CHMO shall set policy and provide oversight of clinical activities.
2.4.2.2 The Director of Health and Medical Systems ensures the appropriate delivery of diagnostic and treatment service through regular periodic reviews.
2.4.2.3 The Medical Director at each NASA Center is responsible for accurate diagnosis, timely treatment, and appropriate follow up of all occupational injuries and illnesses in employees and for reporting all work-related injuries and illnesses to Center personnel responsible for OSHA record keeping.
2.4.2.4 The Medical Director shall monitor occupational injuries and illnesses for trends and provide statistics to Center management for analysis and corrective action, as appropriate.
2.4.2.4.1Any developing trends in occupational injury and illness shall be reported by Center management to the CHMO.
2.4.2.5 Medical staff shall coordinate and communicate with NASA Federal Workers' Compensation injury compensation specialists in providing claim-related documents generated at the Clinic, assisting with an explanation of occupational-related illnesses and injuries for which a claim is being made, and making recommendations about employee return-to-work options.
2.4.3 Process Description
2.4.3.1 The following steps shall be followed by all Centers in diagnosing and treating occupational illnesses and injuries.
a. The occupational health history shall be conducted for the assessment of work-related health problems and include total employment and general health histories, with a review of systems and determination of any preexisting conditions to achieve an accurate medical diagnosis.
b. After a health history is taken, an appropriate physical examination is performed with a detailed specific organ or system examination as related to the chief complaint. Laboratory and radiological testing may be used to complement the history and physical examination and to aid in the diagnosis and treatment of the condition.
NOTE: Pre-approval may be required for procedures not routinely performed in the clinic.
c. The Medical Director, or qualified designee, when the Medical Director is unavailable, shall review the care of patients for appropriateness with current standards of care, utilizing published clinical practice guidelines.
d. The Medical Director, or qualified designee, shall document any inconsistencies with a work-related injury or illness and report these to a safety representative for further evaluation of the injury mechanism and circumstances.
e. An assessment of the workplace shall be performed by medical, environmental health, and/or safety personnel to reinforce the importance of injury prevention and implementation of approved reasonable accommodation.
2.4.3.2 All occupational health practitioners shall become familiar with employees' work and the environment in which they work. In order to better understand specific medical issues and cases, it may be necessary for the medical staff to visit the workplace to better understand the mechanism of injury and evaluate health, safety, and ergonomic concerns.
2.5.1 General
2.5.1.1 Maintaining immunity shall be an integral part of NASA's disease prevention and infection control programs to reduce potential health effects related to exposure to vaccine-preventable infectious agents.
NOTE: The number and types of immunizations required per employee will vary based upon exposure risk.
2.5.2 Responsibilities
2.5.2.1 The CHMO shall establish an Agency immunization policy.
2.5.2.2 The Director of Health and Medical Systems ensures Center immunization policies are in place and the medication management process is sound, properly documented, and meets NASA quality assurance program elements through regular, periodic reviews.
2.5.2.3 The Center Medical Director shall establish immunization policy and procedures and ensure immunization services are available in such areas as international travel, medical surveillance/job certification, occupational injuries/illnesses, and preventive medicine.
2.5.2.4 The Center Medical Director shall ensure the medication management process is sound, properly documented, and meets NASA QA Program elements, and is in compliance with the most current Centers for Disease Control and Prevention (CDC) recommendations.
2.5.3 Process Description
2.5.3.1 Employees with a reasonable risk of occupational exposure to vaccine-preventable diseases such as tetanus, Hepatitis A, or B shall be offered appropriate vaccinations if they lack documented immunity. A declaration form, signed by each employee who declines the Hepatitis B vaccination, is required as an element of prevention against exposure to bloodborne pathogens.
2.5.3.2 Tetanus and diphtheria status shall be reviewed during each patient encounter and immunization given, if the time since the last immunization exceeds the current guidelines, for all employees with tetanus prone injuries at work and those requiring routine boosters.
2.5.3.3 The patient shall be provided an opportunity to discuss any questions about the immunization procedure prior to vaccine administration.
2.5.3.4 An immunization record shall be maintained for each employee and reviewed as part of each patient encounter.
2.5.3.4.1 The record shall reflect documented disease and immunization histories, as well as immunizations administered during employment, and updated at each immunization encounter.
2.6.1 General
2.6.1.1 The exact roles and responsibilities of Center OH disciplines shall be determined by the specific needs at each of the NASA Centers and Facilities.
2.6.1.2 In addition to the Center-wide plan, each clinic shall address emergency preparedness specific to their structure and operations.
2.6.2 Responsibilities
2.6.2.1 The CHMO shall provide technical support and policy guidance to the Center Medical and Environmental COR to effectively negotiate and delineate the roles and responsibilities of NASA OH in relation to the Center-specific Emergency Management Plan.
2.6.2.2 The Director of Health and Medical Systems ensures clinics have addressed emergency preparedness specific to their structure and operations through regular periodic reviews.
2.6.2.3 The COR, or designee, shall keep the Director of Health and Medical Systems current on any Center specific emergency events or any significant modifications to the Emergency Preparedness plan as they relate to OH roles and responsibilities.
2.6.2.3.1 The COR shall serve as an advocate for OH disciplines to ensure assigned roles and responsibilities are sound, obtain management support as needed, and keep the lines of communication viable between the stakeholders. In essence, the COR serves as a liaison between the Center Emergency Operations and the OH team.
2.6.2.4 The Center Medical Director, depending on the extent of medical operations engagement in the Center-wide response plan, shall ensure that the clinic staff is appropriately trained and adequate supplies are readily available.
2.6.2.5 Center OM clinics shall have emergency preparedness policies and procedures in place for emergency operation of the clinic and support of the Center Emergency Management Plan.
2.6.2.5.1 The OM clinic roles and responsibilities shall be integrated into the Center Plan.
2.6.3 Process Description
2.6.3.1 The CHMO shall provide guidance documents and contribute suggestions to improve the medical response.
2.6.3.2 The Center Medical Director shall:
a. Establish procedures to meet the medical expectations of the EP plan including, but not limited to, skill mix and number, personnel training and drills, equipment, and supplies.
b. Establish measures to safeguard and retrieve medical records in paper or electronic format as per Privacy Act, Health Insurance Portability and Accountability Act (HIPAA) and NASA Records Management requirements.
c. Support other OH disciplines in meeting their respective requirements in disaster management such as supporting the EAP in Critical Incident Stress Management training and debriefing.
2.6.3.3 The COR shall ensure the following elements are accomplished:
a. The OH roles and responsibilities in the Center-wide plan shall be reasonable and clearly stated;
b. OH disciplines shall be fairly and consistently represented in the planning process and in drills and simulations with their comments and concerns considered for incorporation into the plan; and
c. Management support shall be solicited for appropriate funding for supplies, staff training, and skill mix and number.
2.7.1 General
2.7.1.1 Each NASA onsite medical clinic shall support the Center in formulating their Continuity of Operations Plan (COOP) Emergency Management Plan.
2.7.2 Responsibilities
2.7.2.1 The CHMO is responsible for providing technical support and written policy direction to OH personnel in support of Center Emergency Management Plans.
2.7.2.2 The Director of Health and Medical Systems ensures support is provided to Centers in formulating their COOP Emergency Management Plan and clinics have programs in place to direct OH personnel in support of Center Emergency Management Plans through regular periodic reviews.
2.7.2.3 The Center Medical Director is authorized to provide expert consultation to the COOP manager and Center management on related public health and medical issues.
2.7.3 Process Description
2.7.3.1 To ensure appropriate action in a pandemic, each Center clinic shall support formulation of a Center-specific COOP plan which should be designed as an addendum to the Center's Emergency Management Plan. The COOP can be an annex to the master Emergency Management Plan or a stand-alone plan.
2.7.3.2 Communication with HQ Emergency Management shall be maintained throughout all phases.
2.8.1 General
2.8.1.1 Medical surveillance protocols shall be used at all NASA Centers and Facilities. The Physical Examination Matrix (Appendix C) provides the examination procedure basics of the most routine and specialty examinations performed at NASA Centers and Facilities.
NOTE: The six categories of physical examinations provided at NASA clinics are listed in Appendix C, Physical Examination Matrix. Due to the potential for changing requirements of an actual examination protocol, the latest content of Agency-provided examinations will be maintained on the Agency OH Web site to ensure currency.
2.8.2 Responsibilities
2.8.2.1 The CHMO shall be responsible for establishing policy, providing requirements and oversight, and reviewing Center physical examination programs.
2.8.2.2 The Director of Health and Medical Systems shall ensure oversight of Center physical examinations through regular periodic reviews.
2.8.2.3 The Center Medical Director shall be responsible for the overall quality of care of all clinic providers.
2.8.2.3.1 In all situations where the decision regarding medical qualification or certification is unclear, the Center Medical Director, or qualified designee when the Medical Director is unavailable, shall review the clinical information and make the final decision.
2.8.2.4 The evaluating physician shall be responsible for interpreting all physical examination test results and determining their significance. If the examinations are not performed onsite, the Center Medical Director, or qualified designee, when the Medical Director is unavailable, reviews the results before final clearance is issued to perform the required task. The evaluating physician is responsible for the preparation of any required "Health Care Professional's Written Opinion" for the pertinent standard, within the specified timeframe.
2.8.3 Process Description
2.8.3.1 Placement of employees in the various physical examination programs is determined by job category, workplace surveys, and specific exposure events.
2.8.3.2 Special Administrative Examinations and health maintenance examinations are offered according to Agency and Center policies.
2.8.3.3 Typically, workers are placed in medical surveillance whose jobs are associated with exposures to hazards with regulatory requirements established by OSHA or NASA.
2.8.3.4 Some programs have specific guidance for placement (e.g., asbestos, organophosphates pesticide workers, hearing conservation, and radiation workers).
2.8.3.5 If insufficient monitoring data or no data is available, individuals shall be placed in medical surveillance based on potential exposures and job title. When this occurs, individuals need to be reassessed as work site monitoring data become available.
2.8.3.6 When an employee is no longer actively exposed to a hazard, as confirmed by the supervisor, the employee shall be removed from that medical surveillance group unless the physician determines the employee should remain in a monitoring status.
2.8.3.7 The Center clinics shall meet the protocol requirements for the following job categories:
a. Specific Potentially Hazardous Exposures;
b. Hazardous Environments/Workplace Examinations;
c. Certification Examinations;
d. Flight Activities;
e. Special Administrative Examinations; and
f. Voluntary Health Maintenance Examinations.
2.8.3.8 Physical examinations shall conform to the requirements delineated in the Physical Examination Matrix (Appendix C), the NASA Aviation Medical Certification Standards, and the pertinent Federal regulations.
2.8.3.9 The frequency of the physical examinations varies and includes:
a. Baseline Examinations:
(1) These examinations shall be ideally performed before the employee starts work in a position with a potential for hazardous exposure.
(2) These examinations provide information necessary to determine if the employee is qualified to perform the job. It also provides a baseline against which changes can be compared.
(3) Baseline examinations and certifications shall be performed prior to engaging in any activity that could be hazardous to the employee or other employees working near or adjacent to them or in contact with them.
b. Periodic Examination:
(1) This examination shall be performed periodically during the time that a worker is employed in a job requiring an examination.
(2) The frequency and extent of periodic examinations vary depending on the work being performed, pertinent regulations, findings from previous examinations, the history of exposure, and/or the age and gender of the workers.
c. Variable or Exposure-Determined Examinations:
(1) These examinations shall be conducted in response to a specific hazardous exposure incident and prompt the examination of all individuals with the suspected exposure, not just those already in the surveillance program.
(2) These examinations may vary significantly from routine medical surveillance protocols, are usually exposure specific, and include biological monitoring tests.
d. Exit/Reassignment Examination:
(1) This examination shall be performed when the worker terminates employment or the job position or is permanently removed from a position which has a potential for hazardous exposure.
(2) Documentation of the worker's state of health at the termination of employment or exposure is essential for comparison purposes if the worker later develops medical problems that could be attributed to past occupational exposures.
(3) This examination is not required if a periodic examination has occurred within the prior six months.
2.8.3.10 If a physical examination has been conducted within the previous six months and has been duly recorded in the employee's health record, it may, at the discretion of the examining physician, be accepted in whole or in part as the requested medical examination.
2.8.3.11 A physical examination conducted for one purpose shall be valid for any other purpose within the prescribed validity period if that physical contains the proper data.
2.8.2.11.1 If the examination is deficient in scope, only those tests and procedures necessary to meet the additional requirements shall be performed.
2.8.2.11.2 The results shall be recorded and appropriate approval provided by the examining physician.
2.8.3.12 A clear determination of "Medically Qualified" (or "Medically Certified") or "Medically Disqualified" (or "Not Medically Certified") shall be made.
2.8.3.12.1 As appropriate for the type of examination, any limiting factors or restrictions shall be noted so that reasonable accommodation for employees may be considered by the Agency as required by the Americans with Disabilities Act, the Rehabilitation Act, and NASA Policy on Reasonable Accommodations (NPR 3713.1).
2.8.3.13 If additional tests or other actions are needed for qualification or certification
(e.g., failed vision because corrective lenses are not available, additional tests are needed, or a temporary condition exists like a cold or the flu) and the condition represents a potentially immediate hazard to the employee, fellow employees, or the success of the project/mission, the employee shall be placed on a modified duty status.
2.8.3.13.1 A followup appointment shall be made to either qualify or disqualify the employee.
2.8.3.14 Where no written standard has been established for a function, the provider shall use best medical judgment to determine whether a disqualifying impairment exists. The Medical Director is responsible for review and final recommended work status in these cases.
2.8.3.15 Appeal, redress, second opinions, and challenged decisions shall be handled at the lowest level of authority at the Center.
2.8.3.16 When a Standard Written Medical Opinion is required by regulation, except for lead, bloodborne pathogens, and asbestos where the Federal Regulation (29 CFR 1910) shall be consulted; the following format shall be followed:
a. A medical condition has [has not] been detected that would place the employee at an increased risk of material impairment of the employee's health from [Specific Hazard] ______ exposure-related disease or injury;
b. There are no limitations on the employee or on the employee's use of personal protective equipment, including respirators;
c. The employee has been informed of the results of the medical examination and of any medical conditions related to [specific hazard] ____- exposure that would require further explanation, evaluation, or treatment;
d. The employee has been informed of the results of the medical examination and of any other medical conditions not related to [specific hazard] ____-exposure that require further evaluation or treatment; and
e. The employee ______________________ is certified for work as __________ without limitations [or certified to work with the following job or Personal Protective Equipment (PPE) limitations: ________].
Health Care Provider Name: ________________________
Signature: ________________________ Date: _________
2.8.3.17 The employer shall provide a copy of the written opinion to the affected employee.
2.8.3.17.1 Unless otherwise noted, the Standard Written Medical Opinion shall be sent within 14 days of completion of physical examination and receipt of laboratory studies.
2.9.1 Introduction
2.9.1.1 Initial clinic response in an emergency situation shall include the use of a medical defibrillator or an AED, if indicated, in order to stabilize the patient until the emergency transport to appropriate medical facilities arrives.
2.9.1.2 NASA clinics are not designated emergency facilities and do not provide emergency medical care as part of their regular scope of services. After stabilization, Emergency Medical Services (EMS) shall always transport emergent patients to the nearest appropriate emergency facility, never to a NASA clinic.
2.9.2 Responsibilities
2.9.2.1 The CHMO shall provide policy guidance and technical support to ensure that all NASA Centers and Facilities have emergency medical response capability that is consistent with published guidelines.
2.9.2.2 The Director of Health and Medical Systems shall ensure appropriate occupational health response in an emergency medical situation through regular periodic reviews.
2.9.2.3 The Center Medical Director shall provide oversight of all NASA and NASA-contracted EMS providers. This oversight involves administrative and medical review of all runs, provision of standing orders, and ensuring that the EMS are adequately staffed and equipped and comply with all NASA, state, and local EMS requirements as practical given contract and locality-specific requirements.
2.9.2.4 The Center Medical Director shall collaborate with Center safety and security leadership to ensure a First Responder Program that includes AED capability according to the Center-wide AED Policy.
2.9.3 Process Description
2.9.3.1 The EMS for each Center shall comply with the following minimal requirements:
a. EMS shall comply with all state and local regulations for ambulance and EMS requirements;
b. Advanced Life Support capability shall be required with a response time within eight (8) minutes, at least 90 percent of the time;
c. First responders with AED capability shall have a response time of four (4) minutes or less for most Center personnel; and
d. The EMS provider at each NASA Center and Facility shall participate in the Center-wide Emergency Response Plan, under the direction of the on-scene incident commander.
e. EMS providers shall participate in emergency drills and exercises to enable full understanding of their responsibilities within the Emergency Response Plan.
2.10.1 General
2.10.1.1 All Centers shall have an AED program which implements the requirements contained in this section.
2.10.2 Responsibilities
2.10.2.1 The CHMO shall establish the NASA AED policy and program requirements.
2.10.2.2 The Director Health and Medical Systems shall ensure compliance with AED policy through regular, periodic reviews.
2.10.2.3 The Center Medical Director shall provide oversight and medical direction for the Center AED program.
2.10.3 Process Description
2.10.3.1 The Center shall complete a formal assessment of the site to determine the appropriate number of AEDs needed, where they should be located, based on population and demographics, layout of facilities, and level of risk in the facility environment, allowing for an optimal response time.
2.10.3.2 The Center shall have a written Center-wide AED program that includes roles and responsibilities, medical equipment and supplies, operational protocols, equipment maintenance, responder training and drill requirements, and a quality assurance plan.
2.10.3.3 The Center AED program shall be integrated with the Center Emergency Response Plan or as an appendix to that plan.
2.10.3.4 The written Center AED program plan shall be reviewed at least annually.
2.11.1 General
2.11.1.1 In developing a Center-specific Bloodborne Pathogens (BBP) plan that addresses the requirements of the BBP Standard (29 CFR 1910.1030), the following requirements shall apply:
a. Center plans may differ based on additional state and local requirements.
b. The BBP plan must be acceptable to the CHMO and contain the primary requirements of the OSHA BBP Standard, 29 CFR 1910.1030, Bloodborne Pathogens.
c. The BBP plan shall be reviewed annually, as needed, to ensure currency.
2.11.2 Responsibilities
2.11.2.1 The CHMO shall provide guidance and technical support for the development and implementation of the Center-wide BBP plan.
2.11.2.2 The Director of Health and Medical Systems ensures Center occupational health programs have current BBP plans through regular periodic reviews.
2.11.2.3 The COR, or designee, shall require medical personnel to establish a written, Center-wide BBP plan that identifies at-risk workers (those with reasonable risk of exposure).
2.11.2.3.1 The COR, or designee, shall ensure that the Center operations are in compliance with the plan's requirements and the plan addresses the following issues:
a. A culture of open communication among Directorates and disciplines such as medical, IH, facilities operations, training coordinators, supervisors, and safety personnel;
b. Active participation in both the development and implementation phases is essential;
c. Consistent documentation and record keeping of all the requirem`ents such as training, medical surveillance and immunization, biohazardous waste, and post exposure prophylaxis; and
d. Enforcement of medical confidentiality and security of health information as per Privacy Act requirements and where applicable to the HIPAA.
2.11.2.4 The Center Medical Director shall establish policies and procedures to ensure compliance with the BBP plan and that treatment is available for all employees in the event of an actual exposure in compliance with the OSHA BBP Standard. This may include but is not limited to:
a. Providing oversight for the content and/or delivery of related training classes;
b. Provision and documentation of Hepatitis B vaccine to the at-risk employees free of charge;
c. Documentation of declination of offer to vaccinate and the process by which the employee may obtain the vaccine at a later date;
d. Post exposure prophylaxis plan;
e. Medical confidentiality; and
f. Issuing the medical opinion letter in compliance with the BBP Standard.
2.11.2.5 The Medical Director and the COR or designee shall jointly establish a process by which they can address any deviations from the Center Plan and review the plan annually in collaboration with the affected Directorates and disciplines.
2.11.2.6 Center OH personnel shall be a resource and assist in writing the Center BBP plan.
2.11.3 Process Description
2.11.3.1 The CHMO shall communicate guidance documents via the Agency OH Web site and provide oversight and evaluation of the BBP plan during the review process.
2.11.3.2 The COR, or designee, shall actively participate in the development and implementation of the written Center-wide BBP/Exposure Control Plan(s) and ensure collaboration between the disciplines, especially when more than one contractor or tenant organization is involved.
2.11.3.2.1 The COR, or designee, shall also advocate for a work environment conducive to the success and consistent application of the plan.
2.11.3.3 The plan must address methods of compliance with universal precautions, engineering and work practice controls, PPE, housekeeping, and bio hazardous waste processing.
2.11.3.4 Medical surveillance and evaluation shall include the offer of Hepatitis B immunization, declination of offer to vaccinate (if applicable), post exposure evaluation and treatment, necessary followup, and issuance of the written medical opinion letter.
2.11.3.5 The Center Medical Director shall specify in the plan the means to protect and train the at-risk employees.
2.11.3.6 The plan must be made accessible to the employees and should serve as the foundation of the respective employer's plan.
2.12.1 General
2.12.1.1 NASA Centers shall institute a systematic, coordinated, and continuous infection control program that focuses on surveillance, prevention, and control of infections.
2.12.1.2 Center programs shall encompass activities at the direct patient care level and at the patient care support level to reduce risks of nosocomial/clinic-acquired infections in patients.
2.12.1.3 Activities shall also be designed to reduce risks of transmission of infections among civil service personnel, contractors, health care personnel, students, and visitors.
2.12.1.4 Particular focus for infection control shall be placed on direct patient care practices, ancillary services, such as laboratory, radiology, and rehabilitation, support services, such as linen supply, and fitness centers.
2.12.1.5 OH personnel shall use the checklist from the Agency OHP Web site to facilitate implementation and assessment of infection control. The checklist is on the Policies page under Documents, Guidelines, and Checklists.
2.12.2 Responsibilities
2.12.2.1 The CHMO shall establish an infection control program policy which includes oversight and evaluation of OH infection control programs.
2.12.2.2 The Director of Health and Medical Systems shall ensure Centers have current infection control plans through regular, periodic reviews.
2.12.2.3 Center Chief Medical Officers/Medical Directors shall ensure that an infection control program is established and maintained at their Centers. These officials are responsible for ensuring that adequate resources, including time and training, are available to support the program.
2.12.2.4 The infection control program shall be the responsibility of at least one person designated by the Center Chief Medical Officer/Medical Director. That individual is known as the Infection Control Officer (ICO) and is responsible for overseeing the program.
2.12.2.4.1 Specific knowledge and training relevant to infection control shall be sufficient to enable the designated person to keep up to date on regulatory changes.
2.12.3 Process Description
2.12.3.1 The designated ICO shall establish, maintain, and oversee an Infection Control Plan and an Infection Control Committee (ICC) consisting of a physician, a nurse, and any additional staff necessary to manage the program effectively. The ICC should coordinate all activities related to the surveillance, prevention, and control of nosocomial infections.
2.12.3.2 The Center ICO and/or ICC shall develop, implement, and maintain an Infection Control Plan that includes program goals, surveillance activities, infection control guidelines, infection control training, nosocomial/clinic-acquired infections reporting process, program assessment, performance improvement procedures, and program documentation.
2.12.3.3 The Infection Control Plan shall be reviewed based on the proceeding year's infection control data by the ICO/ICC. The review should include infectious waste disposal, shelf life of all stored sterile items, reprocessing of non-disposable items, housekeeping contract, linen services, radiology, and laboratory services.
2.12.3.4 The infection control guidelines and practices address patient care issues such as hand-washing practices, approved antiseptics and disinfectants, sterilization of equipment and disinfecting the clinic, laundry, housekeeping, ventilation, and environmental sampling. There shall be a medical surveillance program for the health care personnel, including immunizations, post-exposure protocols, and work restrictions/accommodations. The Center BBP Plan and a tuberculosis prevention and control plan are also included as part of the guidelines and practices. The infection control guidelines and practices must be reviewed and updated every three (3) years by the ICO/ICC.
2.12.3.5 Infection control issues and data, including infections and communicable diseases, immunization status of health care personnel and tuberculosis skin testing conversion data, shall be reviewed and summarized on a regular basis by the ICO or ICC to determine if trends are being formed. Appropriate action must be taken on all infection control issues or problems and a process for followup established to ensure effectiveness of the corrective action.
2.12.3.6 To ensure compliance with infection control standards, the ICO and/or the ICC shall conduct facility inspections at least annually.
2.12.3.7 The ICO shall ensure that all health care personnel and facilities comply with applicable Federal, state, and local regulations, including notification of the public health agency when patients or health care personnel are treated for infectious or communicable disease.
2.12.3.8 The training of health care personnel on infection control methods is required by Federal (OSHA) regulations. For infection control, the training shall include the following:
a. Newly assigned health care personnel shall receive infection control training within ten working days of placement in the clinical environment;
b. Health care personnel shall receive infection control training, including OSHA BBP, universal precautions, and Personal Protective Equipment (PPE) training, annually;
c. Health care personnel shall receive training when significant regulatory changes occur; and
d. Health care personnel providing direct care to patients shall receive continuing education on patient care practices to minimize the risk of nosocomial-acquired infections.
2.12.3.9 Personnel shall have copies of training materials, general information, and infection control reference materials available to them. All training documentation and continuing education records must be kept in the health care personnel records in accordance with NASA records management guidelines.
2.13.1 General
2.13.1.1 All NASA Centers shall adhere to the requirements for Medical Record Management established in this section, NPR 1850.1, Quality Assurance of the NASA Medical Care System, Chapter 3, Medical Quality Assurance Records, and the Records Management Plan for the NASA Electronic Health Record System.
2.13.2 Responsibilities
2.13.2.1 The CHMO shall establish medical information management policy and evaluate the Centers' medical information management policy and procedures.
2.13.2.2 The Director of Health and Medical Systems shall periodically conduct a review of Centers' medical records management policies and procedures through the regular review process to ensure the Electronic Health Record System (EHRS) meets Privacy Act and NASA records management requirements.
2.13.2.3 The OH COR is responsible for ensuring that the clinic has proper resources and systems in place to meet the Agency's requirement for management of medical information and record retention.
2.13.2.4 The Center Medical Director shall ensure the clinic has a medical information management policy that encompasses the requirements of the Records Management Plan for the NASA Electronic Health Record System.
2.13.2.5 Center clinical personnel shall maintain accurate and complete patient medical records and ensure the security and confidentiality of those records.
2.13.3 Process Description
2.13.3.1 Each Center shall use the designated Agency EHRS in accordance with NASA records management requirements unless an OCHMO waiver is approved.
2.13.3.1.1 In all cases, electronic health data shall be made available to the Agency electronic health database.
2.13.3.2 An individual medical record shall be established and maintained beginning with the first patient encounter.
2.13.3.3 The medical record documentation shall include sufficient information to identify the patient, patient medical history, reason for visit, subjective and objective findings, assessment, and plan written in the Subjective Objective Assessment Plan format. In addition, the medical record may include:
a. Patient demographics;
b. History and medical questionnaires;
c. Work-related injury and illness reports;
d. Environmental hazards or conditions;
e. Occupational exposures and incidents;
f. Summary Sheet;
g. Consultation reports;
h. Signed informed consent;
i. Laboratory test and x-ray results;
j. Immunizations;
k. Medication(s) provided or prescribed;
l. Allergies; and
m. Referrals to community healthcare providers.
2.13.3.4 Medical records shall be maintained and safeguarded in accordance with all Federal and state laws or regulations, NASA's record requirements, and this NPR, including the following:
a. Occupational Safety and Health Administration (OSHA); and
b. NPR 1850.1, Quality Assurance of the NASA Medical Care System.
2.13.3.5 The Center shall have medical record policy and procedures addressing access to medical records, release of records and to whom, copying of records, and privacy and confidentiality in compliance with 14 CFR Part 1212 and other applicable Federal and state laws and regulations.
2.13.3.6 The Center shall have a policy on managing sensitive health information per Privacy Act requirements.
2.13.3.6.1 The policy shall address the separate storage of those records and/or coding to preclude direct identification of the patient. Sensitive health information includes all EAP records, mental health, chemical dependency, sexually transmitted diseases, and drug and alcohol test results.
2.14.1 General
2.14.1.1 The potentially detrimental impacts of unusual shifts and prolonged work-times shall be given a high priority by all NASA Centers to prevent worker psychological and physiological stress and undesirable outcomes. Safe work practices that minimize human error factors, especially fatigue, require safe work-rest cycles and shift scheduling.
2.14.1.2 Work-rest cycles shall take into consideration and make proper allowances for the work environment, including temperature extremes. The processes presented below are provided to ensure safe work practices and mission success.
2.14.1.2.1 In situations where there is conflict between NPR 1800.1 and Aviation operations policies, the latter shall supersede the requirements contained herein.
2.14.1.3 The criteria are provided for Critical and Non-Critical positions as follows:
a. A Critical Position is one in which the worker's job performance can directly impact ground safety, flight safety, or mission success. This may include, but is not limited to, workers who:
(1) Deal directly with flight hardware, software, or ground support equipment;
(2) Have authority to make decisions regarding flight hardware or software processing;
(3) Are involved in launch and landing activities;
(4) Work in ground systems with physical or functional interface with flight systems;
(5) Work with hazardous sequences or procedures; and
(6) Work on systems with minimal or no checks and balances related to employee decisions
or actions.
NOTE: Personnel who are in Critical roles on a part-time basis will be considered to be in a Critical Position on a full-time basis for purposes of work-rest cycle limitations.
b. All other positions are considered to be Non-Critical.
2.14.2 Responsibilities
2.14.2.1 Center Directors and Senior Managers shall ensure that policies regarding work-rest cycles, implementation of work-rest cycles, maximum work limits, and shift schedules as required for routine and extended or emergency work scenarios are adhered to.
2.14.2.1.1 These policies shall also establish those positions designated as Critical for each Center or Facility.
2.14.2.2 The CHMO shall issue relevant policy and directives and provide supporting advocacy and resources.
2.14.2.3 Center OH staff shall provide assistance in policy development and professional consultation to managers and supervisors regarding requirements for standard and prolonged work schedules and work excesses. Supervisors should seek out fatigue risk management expertise, as necessary.
2.14.2.4 Managers and supervisors shall ensure that all duty hours are recorded and counted toward the maximum work periods identified below.
2.14.2.4.1 Managers and supervisors shall also report any work-rest cycles that are not within the established policies to the designated management level for risk assessment and approval of deviations, given the current work requirements. Work time data must be available for review.
2.14.2.5 Center EH Managers assure that potential exposures are appropriately evaluated and that OELs are adjusted, as necessary, from the 8-hour time-weighted average to reflect actual conditions and work shifts.
2.14.3 Process Description
2.14.3.1 For Non-Critical Positions, employees shall not work in excess of the following maximum work times (MWT):
a. 12 consecutive hours (16 consecutive hours in emergency situations with approval);
b. 60 hours during a seven (7) day work week;
c. Seven (7) consecutive days without at least one (1) full day off;
d. 240 hours during a four (4) week period; and
e. 2,500 hours during a rolling 12-month period.
2.14.3.2 Deviations from these maximum work times require approval by a designated supervisor.
2.14.3.3 For Critical Positions, employees shall not work in excess of the following MWTs:
a. 12 consecutive hours (16 consecutive hours in emergency situations with approval by
a supervisor capable of evaluating the human factors risk level for the Critical role. Only during a Center or Program Declared Emergency may 16 consecutive hours be exceeded with high level of designated approval);
b. 60 hours during a 7 day work week*;
c. Seven (7) consecutive days without at least 1 full day off* (deviations may be pre-approved at a high level for up to 18 consecutive days with 2 full days off required after the extension period);
d. 240 hours during a 4-week period*; and
e. 2,500 hours during a rolling 12-month period*.
NOTE: The asterisks (*) denotes pre-approval is required for deviations by a designated supervisor after consideration of human factors safety issues for the Critical Position.
2.14.3.4 Overtime may be required because of a problem during operation or because of an extended work process. In either case, overtime shall not exceed the stated guidelines.
2.14.3.5 For Center or Program Declared Emergencies, maximum work times shall only be exceeded with approval at the Deputy Center Director level or equivalent designee.
2.14.3.5.1 Each Center shall have the capability to cover unexpected absences satisfactorily without having individuals work more than 12 hours per day.
2.14.3.6 Emergency or extremely unusual circumstances can require work performance essentially at endurance capacity. This shall be invoked only for life-threatening emergencies, natural disasters, mass casualty accidents, or war.
2.14.3.7 Workers performing prolonged routine shifts shall receive training related to the adequate sleep times required between shifts.
2.14.3.8 The calendar year, the week, and the calendar day (which changes at midnight) shall be used for work time evaluation and maintenance of accurate time records.
2.14.3.9 Under no circumstances shall an employee be required to work such that there is not at least eight (8) hours off duty between shifts. A minimum of ten (10) hours off duty is preferred and 12 hours or more is optimal to accommodate employee commute time and domestic and sleep needs.
2.14.3.10 When the 8-hour period is shifted within the 24-hour day-night cycle (shift work), compensatory time must be allowed for circadian rhythms to adapt. Forward rotating shifts, from day to evening to night, rather than counter to it are easier for human adaption.
2.14.3.11 The traditional "standard" 5-day, 8-hour shift is becoming frequently replaced with consecutive 10 or 12-hour shifts, compensated to the worker by more time/days off. The basic 12 hour/day schedule shall be "2-on, 2-off," "3-on, 3 off," or "4-on, 4-off." Three consecutive 12-hour shifts are optimal. Working more than 4 consecutive 12-hour shifts is associated with excessive fatigue and strongly discouraged since it may result in significant impact on performance of duties, mission, and safety.
2.14.3.12 Time zone changes alter or shift natural bodily rhythms and require considerable time to reach new equilibriums as evidenced in the well-known "jet lag" syndrome. Consideration shall be given to allowing for adaptation times to avoid critical decisions in a chronobiologically impaired state. Circadian rhythms affect physical ability, mental alertness, decision making, and overall well-being that can predispose to injury and adversely impact work capacity, quality, and safety.
2.14.3.13 To minimize worker stress and fatigue related to time factors, the following procedures shall be followed:
a. Define the "standard" work period for all operations and tasks, including method of shift rotation if required, as well as breaks and required rest cycles;
b. Clarify responsibilities, work expectations, and desired outcomes for any process or decision;
c. Minimize negative consequences of shifting work times by:
(1) Having employees select preferred shifts consistent with mission needs.
(2) Considering individual circadian rhythms to insure adequate work and sleep-rest
cycles.
(3) Allowing adequate time for adaptation and recovery from old to new shift or time
zone.
(4) Understanding the "criticality" of the work to evaluate risk of physiological and
psychological consequences of chronobiological stress.
d. Defining "critical job categories" and assure that employees assigned to these categories understand the full implications of the work schedule and rest cycles. Educate employees about the importance of adequate rest for safe job performance;
e. Defining "extended" work periods for job categories;
f. Allowing "deviations" from standard maximum work requirements by the following criteria:
(1) Need, urgency, and benefit.
(2) Risk assessment.
(3) Prior anticipation of extended work schedules or deviations from guidelines
shall be noted in position descriptions; and
g. Provide an impartial council (e.g., HMTA or the Agency DASHO) to hear and resolve disagreements related to work schedules, shift work, and rest cycles.
2.14.3.14 Maintain accurate records of work schedules and hours actually worked.
2.14.3.15 Adjustment and application of OEL's to unusual shifts shall be determined by a qualified industrial hygienist using the Brief and Scala model or other acceptable models as described in Patty's Industrial Hygiene and Toxicology.
2.15.1 General
2.15.1.1 In offering health services to NASA employees preparing to embark on international travel or assignment, the requirements of this section shall be followed in order to reduce the risk of illness or injury, prevent loss of productivity, and safeguard their health.
2.15.1.2 It is solely the traveler's responsibility to contact the NASA clinic four to six (4-6) weeks prior to scheduled travel departure to allow adequate time for vaccines, if needed.
2.15.2 Responsibilities
2.15.2.1 The CHMO shall establish international travel health policy.
2.15.2.2 The CHMO shall maintain a contract to provide medical evacuation and assistance to NASA civil service employees traveling internationally on official government-related business.
2.15.2.2.1 The contract maintained by the CHMO shall include travelers' ability to instantly access destination-specific travel information, travel health alerts, pre-departure checklists, and other resources via the vendor's Web site or Web-page that has been customized for NASA.
2.15.2.2.2 NASA Centers may employ additional medical evacuation/service vendors to assist civil service personnel on official Government foreign travel. Civil service employees who become injured or ill during official Government travel may be eligible for coverage by the Federal Employees Compensation Act and should consult with their Center's injury compensation specialist for assistance as soon as possible.
2.15.2.3 The Director Health and Medical Systems ensures proper execution of clinic travel policy through regular, periodic reviews.
2.15.2.4 Each Center's Foreign Travel Coordinator shall be familiar with the Agency's medical services and evacuation contract so that travelers can be notified of the method of accessing the vendor's Web site.
2.15.2.5 International travel services provided by occupational medical clinics shall be consistent with the current CDC Health Information for International Travel "Yellow Book."
2.15.2.6 The Agency's contract provisions shall also apply to NASA civil service employees who are in the midst of, or have completed, international permanent change of station activities.
2.15.3 Process Description
2.15.3.1 NASA OM clinics shall establish policy and procedures for providing travel medicine services for Center personnel going on official Government foreign travel or assignment.
2.15.3.2 NASA OM clinics shall have access to current relevant information on international travel including, but not limited to, the CDC, World Health Organization (WHO) health information for international travel, Travel Health Notices, and the U.S. Department of State.
2.15.3.3 International travel services to be offered shall include the following elements:
a. General pre-travel briefing and information;
b. General health risk assessment (An assessment of the employee's potential risk for illness considers any underlying medical problems, immunization history, allergies, current medications, previous travel, and travel destination.);
c. Immunizations;
d. Traveler's diarrhea information and advice;
e. Malaria risk assessment and advice, if appropriate;
f. Air travel and health information (includes addressing circadian rhythm adjustment);
g. Destination safety information (e.g., protective and preventative health advice, as appropriate to the destination risks);
h. Travel kits, in accordance with NASA Center policy;
i. Pre-travel evaluation of any work-related environmental health issues/concerns, identification of PPE or training needs shall be provided by the employee's appropriate supervisor;
j. Medical surveillance or job-certification examinations; and
k. Other sources of health-related information including:
(1) The Web site address for NASA's international medical evacuation and assistance vendor and the name, phone number, and e-mail address for the CHMO's point of contact for employees' assistance with Web site access and Agency assistance before and during travelers' international business travel; and
(2) Post travel follow up scheduling and advice, as required.
2.15.3.4 Centers are authorized to discuss and offer international travelers the CDC required and recommended immunizations for the country of destination.
2.15.3.5 Depending on the destination, pre-travel confirmation of the Tuberculosis (TB) intra-dermal skin test status with Purified Protein Derivative may be required. Centers shall follow the CDC guidance on followup for positive results and post-travel evaluation of skin test status for those who traveled to areas where there are high incidences of TB.
2.15.3.6 Centers are authorized to assemble and issue travel medical kits to NASA employees traveling on official Government business. The instructions and contents of the medical kits shall be determined by the Center medical director.
2.15.3.6.1 A summary of the traveler's past and any current medical history, including allergies, medications, and special diet shall be provided to the traveler in accordance with privacy and confidentiality requirements.
2.15.3.7 Medical services for all non-NASA-related travel are the responsibility of the employee.
2.15.3.8 NASA contractors are responsible for establishing their medical clearance policies and facilitating arrangements with a medical service provider for their employees, in accordance with their contract. Responsibility for international emergency medical services remains with the contractor and contracted employee, as specified in NASA FAR Supplement, Clause 1852.242-78.
2.15.3.9 Services for civil service employees on official Government foreign travel who suffer an injury or illness can be obtained using the Agency's medical evacuation assistance contractor. Examples of these services include medical and dental referrals/assistance, prescription medicine assistance, and local transport to medical facilities. NASA civil service employees who suffer a traumatic injury or occupational illness while in the performance of their official duties may also be eligible for compensation benefits under the Federal Employees' Compensation Act. All mishaps must be reported in accordance with NPR 8621.1, NASA Procedural Requirements for Mishap Reporting, Investigating, and Recordkeeping.
3.1.1 General
3.1.1.1 To promote a healthful work environment with commitment to the physical and mental health and productivity of its workforce, NASA Centers' Primary Prevention and Health Promotion programs shall be designed to increase awareness through education, foster lifestyle and behavioral modification, and create a supportive work environment.
3.1.2 Responsibilities
3.1.2.1 The CHMO shall establish policy requirements for primary prevention programs.
3.1.2.2 The Director of Health and Medical Systems shall develop a primary preventive strategy for the Agency and ensure implementation through the regular, periodic review process.
3.1.2.3 The Center OH COR shall support the implementation of the annual health promotion plan.
3.1.2.4 The Center Medical Director or designees shall implement the annual health promotion plan.
3.1.2.5 The COR and Medical Director shall designate a representative to serve on the Agency HPW.
3.1.3 Process Description
3.1.3.1 The CHMO shall provide direction and guidance towards standardization of majority of health promotion and wellness activities across the Agency based on the following measures:
a. Establish an Agency-wide HPW composed of Center representatives with the charter to standardize health education programs.
b. Establish periodic meetings with the team for the purpose of educational presentations on emerging issues, discussion of new and innovative ideas, development of relevant policies and procedures, and evaluation of the existing programs and campaigns;
c. Identify and coordinate particular campaigns and initiatives for Agency-wide dissemination, including participation in OPM-directed Federal-wide health promotion initiatives;
d. Maintain a section or sections on the Agency OH Web site as an informational portal for health resources;
e. Ensure sources of health education material (Web-based, digital, or printed) in support of identified campaigns and initiatives are disseminated to Center HPWs;
f. Collaborate with leading health resource organizations and other community and national organizations; and
g. Identify evaluation strategies to assess the effectiveness of the health education programs.
3.1.3.2 The Center OH COR shall support the implementation of the Agency primary prevention plan and associated activities at their respective Center.
3.1.3.3 The Center Medical Director or designee shall assess the feasibility of creating a Center specific health promotion workgroup to address issues in a collaborative and systematic manner in order to:
a. Ensure that the Center's health promotion plan is relevant to their population;
b. Ensure an annual health promotion needs assessment is completed for the Center; and
c. Evaluate the impact of the overall primary prevention and health promotion program. Both short- and long-term goals should be established in the planning stages.
3.1.3.4 The Center Medical Director or designee shall gather program evaluation data and report to OCHMO upon request.
3.2.1 General
3.2.1.1 Primary prevention services are the foundation of NASA OH and all NASA Centers shall implement primary prevention services.
3.2.1.1.1 These services shall encompass both health promotion and health protection directed toward enhancing employee well-being and moving toward a state of optimal health, as well as reducing health risks. Health promotion efforts are designed to increase health knowledge and support employee behavior change related to health and safety practices in the workplace and at home. Health protection measures are designed to eliminate or reduce the risk of disease in order to prevent the development of an illness or injury.
3.2.2 Responsibilities
3.2.2.1 The CHMO shall provide policy guidelines and technical support for the Agency primary prevention program and its various components.
3.2.2.2 The Director of Health and Medical Systems shall assess and review primary prevention and health promotion programs through regular periodic reviews.
3.2.2.3 The OH COR shall advocate for adequate resources in support of primary prevention programs.
3.2.2.4 The Center Medical Director shall ensure primary prevention services are planned, implemented, and evaluated.
3.2.3 Process Description
3.2.3.1 The Center Director shall ensure the planning and implementation of worksite primary prevention programs, services, and policies designed to enhance employee well-being and optimal health, as well as to reduce health risks.
3.2.3.2 The Centers shall offer primary prevention/health promotion programs, such as nutrition, fitness, exercise, health motivation, and targeted disease prevention programs, such as injury prevention, health risk assessment, smoking cessation, weight control, stress management, and seat belt use.
3.2.3.3 The Centers shall evaluate the effectiveness of overall primary prevention program efforts on a regular basis.
3.2.4 Primary Prevention Programs
3.2.4.1 NASA's workplace nutrition program shall increase awareness through education and create a work environment supportive of healthy nutrition habits.
a. Center Medical Directors shall implement nutritional awareness and education programs, advocating for a workplace environment supportive of good nutritional practices in collaboration with the food service vendor(s), where possible, and with support of the respective COR.
b. Current nutritional guidelines such as the USDA, the Academy of Nutrition and Dietetics, etcetera, shall be used.
NOTE: Nutritional awareness and education programs may be conducted in partnership with Center Fitness and Health and Wellness programs.
3.2.4.2 NASA's program to prevent skin cancer includes education, administrative controls, and medical screening.
NOTE: The term medical screening does not preclude nor does it imply a full-body screening by a dermatologist or an OH physician.
a. Center Medical Directors shall provide ongoing awareness through health promotion activities, advocate for occupational exposure limitations, and ensure skin evaluations are provided in accordance with current guidelines and recommendations.
3.2.4.3 The implementation of tobacco cessation programs shall be instituted across all NASA Centers and Facilities.
a. The program shall reach out to tobacco users, smokers and smokeless users, assess their interest in quitting, and provide access to intervention programs. Methods to identify users may include specific campaigns or be part of scheduled physical examinations.
b. The program shall include activities to prevent tobacco use among the workforce, including education on tobacco-related health consequences.
c. Center OH COR shall advocate for a work environment conducive to the success of the smoking cessation program an ensure collaboration between disciplines.
d. The Center Medical Director or designee shall work in partnership with related disciplines such as fitness, EAP, and IH, as well as local agencies or non-profits such as the American Lung Association or American Cancer Society to accomplish the goals of the tobacco cessation program.
3.2.4.4 Immunization practices at NASA Centers shall be based on the latest available recommendations from the U.S. Preventive Services Task Force, Center for Disease Control and Prevention, and other leading health professional organizations.
a. The Center OH COR shall advocate for Center operations and budgetary assignment that are conducive to the implementation of the total immunization program, including an annual influenza immunization program.
b. The Center Medical Director shall ensure occupationally relevant vaccines are available. These include as a minimum tetanus (Td or TdAP) and Hepatitis B vaccines. Additional vaccines shall be included based on Center specific occupational exposures and budgetary allocations.
3.3.1 General
Federal agencies are authorized to offer employee health services "to promote and maintain physical and mental fitness and to help prevent illness and disease," including health services and intervention programs such as exercise and weight control. Fitness programs encompass activities such as organized walking events, aerobic exercise classes, weight lifting, yoga, spinning, fun runs, and fitness assessments. All NASA Centers shall have fitness centers/facilities which adhere to the requirements of this NPR (including features such as exercise equipment, areas for group exercise, locker rooms, and other associated amenities). NASA Component Facilities are encouraged to have fitness centers/facilities which would also be covered under the requirements of this NPR. For NASA components with fitness and/or group exercise/aerobics clubs conducted in NASA-maintained space, this Chapter shall apply on an advisory basis as further delineated in Chapter 7.
3.3.2 In maintaining onsite fitness facilities to promote and encourage employee physical activity, center management and supervisors shall encourage and support employee use of the fitness facility and employee participation in health and wellness activities.
3.3.3 NASA Center Fitness Programs shall incorporate the most recent Office of Personnel Management (OPM) recommended (American College of Sports Medicine [ACSM]) industry standards for staffing, facility design, equipment selection and maintenance, and safety.
3.3.4 Fitness Facility Features
3.3.4.1 NASA onsite fitness facilities shall include separate male and female shower facilities and locker rooms; an exercise room/area large enough to accommodate pre-exercise stretching and/or group classes; and a variety of commercial grade indoor exercise equipment such as treadmills, stair climbers, strength training machines, and free weights. NASA Centers shall make efforts to feature some equipment that can be accessed by individuals with physical limitations, including at least one piece of cardiovascular equipment and one piece of Selectorized or variable-resistance equipment.
3.3.4.2 Message and/or bulletin boards shall be used for communication and posting of relevant information about the fitness facility or items of particular interest to members and other Center employees.
3.3.4.3 An automatic external defibrillator (AED) shall be available within a 1.5 minute walk to any place it may be needed.
3.3.4.4 For facilities with saunas or steam rooms, a monitoring/warning system shall be in place to ensure safe conditions are maintained in these environments, along with prominent signage describing user health risks and time limits for use. Fitness facility staff shall instruct members on personal safety in these environments, especially regarding precautions if pregnant, on certain medications, or with heart conditions.
3.3.4.5 For facilities with swimming pools, water-chemistry safety requirements mandated by codes and regulations shall be met, including chemical storage/disposal, and the appropriate safety equipment (e.g., shepherd's crook, safety rope) available at all times.
3.3.4.6 Interior physical activity areas shall have a working clock, a prominent chart/poster of target heart rates, and a prominent chart/poster depicting ratings of perceived exertion to enable users to monitor their activity.
3.3.4.7 A first-aid kit containing bandages, gloves, and a pocket mask shall be maintained and available to the fitness facility staff for emergency use. If any staff or fitness members are expected to deal with, or have exposure to, potentially hazardous materials, including bodily fluids, procedures shall be in place to ensure these activities are conducted according to all applicable regulations and within safety guidelines.
3.3.4.8 A notification system in the fitness facility, featuring prominent signage, instructions, and ease of use shall be available to call medical, first aid, and security. If the emergency system is inoperable or only partly functional, a sign(s) shall be posted at the fitness facility to notify members of the status and the alternative methods to be used to summon emergency assistance. At a minimum, a sign shall be posted with this information immediately next to any device that is not fully functional. Any emergency system that is not fully functional shall either be repaired or replaced as soon as possible.
3.3.5 Fitness Facility Plan Components
3.3.5.1 Center fitness facility plans shall be written, maintained onsite, and periodically reviewed and revised when conditions warrant. The Plan shall serve as a comprehensive document that allows fitness facility management to easily identify information about operations, equipment, procedures, and staff. For convenience, information and documents that frequently change or that are voluminous may be maintained as appendices of the core Plan. At a minimum, plans shall include the following:
a. Location/address of the facility and a map showing emergency exits and location(s) of AEDs;
b. Facility hours of operation;
c. The number and type of staff associated with the facility, as well as their qualifications, certifications, and responsibilities;
d. Identification of other resources, entities, agencies that participate in the program or contribute to its operations (e.g., Center tenants and/or contractors);
e. A description of the methods used to integrate the fitness program with other Center or Agency functions or related programs (e.g., Medical, Safety, Employee Assistance);
f. A description of the methods used to communicate with potential and current fitness facility users to obtain feedback, provide assistance with personal fitness goals, or share information about activities associated with the fitness facility;
g. Member pre-activity screening and orientation procedures;
h. Procedures used to handle broken equipment or equipment that is going to be permanently removed from service; and
i. Emergency response procedures and a description about periodic drills conducted.
3.3.6 Fitness Facility Equipment Maintenance
3.3.6.1 The following activities shall be conducted: (1) maintenance of fitness facility equipment to reduce the number of repairs and extend the life of the machinery; (2) a visual inspection, using a pre-determined checklist at least once per week to identify any broken or unsafe equipment; (3) removal of broken or unsafe equipment or prominent tagging and disabling of equipment to prevent use; (4) development and implementation of a preventive maintenance program for fitness equipment, including formal documentation describing the work performed, the date the work was performed, and the name of the individual or entity that performed the work; and (5) maintenance of equipment inspection and repair records in a log or equivalent and made part of the written fitness facility plan as an appendix.
3.3.6.2 Clean disposable towels/wipes, anti-bacterial cleaning solution or similar supplies shall be available to members to wipe off equipment. Members shall be encouraged to clean hands before and after workouts with soap and water or hand sanitizer and to keep skin lesions covered with a clean, dry dressing.
3.3.6.3 Non-slip floors shall be the standard for all shower and locker room facilities. Floors in the showers and locker rooms shall be cleaned frequently enough to address the presence of mold, mildew, soap scum, and unhealthy conditions resulting from high utilization. Shower curtains shall be inspected regularly and cleaned or replaced whenever there is evidence of mold, mildew, soap scum, or other unsanitary conditions.
3.3.6.4 Sinks, toilets, and urinals shall be regularly cleaned and disinfected on a schedule consistent with conditions in facilities used by a large volume of individuals on a frequent and daily basis.
3.3.6.5 Ventilation grills, vents, and mounted/portable fans in all areas of the fitness facility shall be visually inspected and cleaned to address dust, debris, and dirt build up on the grills.
3.3.6.6 Flooring in fitness facilities shall be conducive to, and appropriate for, activities performed in those areas. Due to the nature of activities performed and the number of people using fitness facilities, floors require cleaning more often than those in office settings. Fitness facility floors shall be cleaned as thoroughly as possible, on a schedule based on facility use, composition, and inspection results.
3.3.6.7 Fitness facilities with saunas, steam rooms, or whirlpools shall ensure that the areas and equipment are maintained, calibrated, and cleaned according to the manufacturer's and industry recommendations.
3.3.6.8 Ice machines, portable water dispensers, and drinking fountains shall be maintained and cleaned according to manufacturer recommendations and relevant sanitation requirements.
3.3.6.9 Free weights, fitness accessory equipment, mats, and similar items shall be thoroughly wiped and cleaned periodically to address sweat, dirt, and buildup from members' use.
3.3.7 Responsibilities
3.3.7.1 Each Center shall identify their fitness facility's primary point of contact to interface and communicate with the Agency Fitness Manager. The point of contact may be the Fitness Facility Manager, Wellness Manager, Fitness Director, and the NASA COR for the fitness facility provider, or other appropriate individual involved in the operation, maintenance, and oversight of the facility.
3.3.7.2 Staff present at a NASA fitness facility shall possess the necessary competencies, certifications, licenses, and credentials for fulfilling their roles and responsibilities to ensure the safety of fitness facility members. Due to the potential of ACSM re-titling categories of professional fitness facility staff, categories are delineated as follows, with the primary importance placed on responsibilities, expertise, and certification: (a) Fitness Manager; (b) Fitness Director; and (c) Group Exercise Trainer/Leader/Instructor.
3.3.7.3 All personnel responsible for daily operation of the fitness facility shall, at a minimum, possess and maintain Cardiopulmonary Resuscitation /Basic Life Support certification and have received Bloodborne Pathogen standard training.
3.3.7.4 At a minimum, the responsibilities of the manager of the fitness facility shall include communicating regularly with the Agency Fitness Manager, ensuring staff certifications and licensure are tracked and updated, ensuring physical environment safety for members, implementing emergency procedures and conducting drills, and ensuring a process is in place for members to receive the appropriate level of medical clearance.
3.3.7.5 The manager of the fitness facility and/or the fitness director are responsible for the overall facility operations, and the fitness director manages exercise and activity programs and supervises staff. The fitness director shall possess a degree in a health and fitness related field or equivalent relevant experience, with at least one year of supervisory experience in the fitness industry and be professionally certified at an advanced level by a nationally recognized health or fitness organization.
3.3.7.6 Fitness staff or others hired to conduct group exercise classes shall, at a minimum, possess current certification in group exercise from the Aerobic and Fitness Association of America (AFAA), American College of Sports Medicine (ACSM), American Council on Exercise (ACE), National Strength and Conditioning Association (NSCA), National Federation of Professional Trainers (NFPT), or a comparable professional organization and have at least six months' experience in conducting group exercise classes. Cardiopulmonary Resuscitation and/or AED certification is required.
3.3.7.7 NASA Centers that provide services in allied health fields such as nutrition or physical therapy shall employ providers who are duly certified, licensed, or registered within their state, as required by law.
3.3.8 Process Description
3.3.8.1 Fitness facilities shall conduct the following: (a) initial screening of new members and annual screening of all members to identify those at risk for a cardiovascular incident while exercising, using at a minimum, the most recent version of the Physical Activity Readiness Questionnaire (PAR-Q) or the health screening questionnaire developed by the Wisconsin Affiliate of the American Health Association; (b) initial evaluation of new members and annual evaluation of all members' blood pressure, with screening results reviewed and interpreted by a qualified health/fitness professional or healthcare professional; (c) referral to either the Center/Facility OH Clinic or member's Private Medical Doctor (PMD) if any results suggest a potential medical problem; with a written medical clearance required prior to the member's use of the fitness facility; and (d) maintenance of members' periodic clearance process status at the fitness facility, with appropriate documents kept according to the rules for Personally Identifiable Information (PII), ensuring that all documents containing specific private medical information (e.g., OH clinic exam results, PMD exam results, doctors notes, etc.) about users are maintained appropriately at the onsite medical clinic.
3.3.8.2 The agency fitness manager, during onsite periodic occupational health reviews, may review general non-medical membership files to ensure quality assurance/quality control.
3.3.8.3 A fitness facility orientation shall be provided to each new member, including a discussion of emergency procedures, fitness facility rules, and detailed instructions on how to safely use the Center and equipment. To ensure consistency, a checklist or similar document will be used by the fitness facility staff conducting the orientation. The orientation shall require a member's signed confirmation that he/she received and understands the information provided. A means shall be available for members to obtain additional information about the proper use of equipment, assistance with their personal fitness program, or a refresher orientation upon request.
3.3.8.4 A mechanism for member comments and feedback shall be implemented (e.g., annual survey for continued quality improvement) to identify concerns, improvements, and quality of the fitness program.
3.3.8.5 A method shall be implemented and enforced to identify (badge, keyed lock) users who have been screened and eligible to use the facility. Users shall sign in manually or electronically each time they use the fitness facility. Centers should make every effort to institute a sign-in procedure process, accomplished through a computerized system in which statistical information can be extracted to monitor fitness facility use.
3.3.8.6 The fitness facility hours of operation shall meet the majority of users' needs and work schedules.
3.3.8.7 For safety and in accordance with General Services Administration (GSA) 41 CFR §102-79.35, OPM guidance, and industry recommendations, unmanned fitness facilities/clubs shall utilize one or a combination of methods to enhance user safety: professional fitness staff; utilization of real-time streaming wide-angle video cameras in fitness facilities with continual monitoring (e.g., fire department, security) during operating hours of the fitness facility; and/or implementation of a policy requiring a buddy system for those using the facility.
3.3.8.8 The installation and implementation of continuously monitored surveillance cameras in fitness facilities shall be considered an additional method for ensuring the safety of members.
3.3.8.9 In a medical emergency, a fitness facility staff member shall remain with the member at all times until assistance has arrived.
3.3.8.10 Fitness facilities shall conduct an emergency drill at least annually to review procedures in place in the event of a medical emergency, manmade/natural disaster, workplace violence, or other critical incident. Documentation of drills shall be maintained at the fitness facility or with the primary POC for the fitness facility. Documentation shall include the date of the drill, names of the participants, the entity/entities involved, and the outcome/critique.
3.3.8.11 Fitness Facility staff AED training shall be conducted as soon as possible after hiring. Training renewal shall be completed by responders based on Federal, state, and local requirements, usually every two years.
3.3.8.12 The Federal Employees Compensation Act (FECA), as amended, 5 U.S.C. S8101 et seq., provides for the payment of workers' compensation benefits to Federal employees sustaining injuries while in the performance of their duties. Civil Service employees using a NASA fitness facility have the right to file a Federal Workers' Compensation claim if they are injured or become ill using the facility. The Department of Labor is the entity that determines whether an injury or illness is compensable.
4.1.1 Program
4.1.1.1 Chapter 4 contains requirements additional to Federal regulatory requirements (e.g., OSHA, NRC, Food and Drug Administration (FDA), Department of Defense (DOD), and Department of Energy (DOE), although some could be enforced under the OSHA general duty clause. The NPR is not meant to replace or repeat those regulatory requirements.
4.1.1.2 In addition to legal requirements, Centers shall comply with applicable consensus standards and proprietary standards (i.e., American Conference of Governmental Industrial Hygienists Threshold Limit Values and Biological Exposure Indices for Chemical Substances and Physical Agents; American National Standard Institute (ANSI); the Society of Automotive Engineers (SAE)).
4.1.1.3 Center EH organizations shall have a direct line of authority to the Center Director, such that other organizations that have conflicting interests in EH decisions are not in the path of authority.
4.1.2 Responsibilities
4.1.2.1 The OCHMO shall establish policy requirements for the EH programs. The OCHMO does not directly oversee day-to-day operations or programs at NASA Centers or other NASA institutions.
4.1.2.2 The Director Health and Medical Systems shall ensure the Center EH policies and programs are assessed for efficacy through regular, periodic reviews.
4.1.3 Recordkeeping
4.1.3.1 Centers shall keep records to evaluate trends and outcomes; validate the effectiveness of EH programs, document training and pertinent EH events, and provide a mechanism for active managerial control over EH programs. These records will be managed in accordance with NPR 1441.1, NASA Records Management Program Requirements.
4.1.3.2 Records shall be complete, accurate, and timely, appropriate for the task, and provide for a continuity of information.
4.1.3.3 Records shall be historically traceable.
4.1.3.4 EH and related records shall be subject to periodic review for quality efficacy and consistency by the OCHMO.
4.1.3.5 Centers shall generate, retain, and dispose of EH records according to NASA records requirements as outline in Section P1d and 1.11 of this NPR.
4.1.3.6 The Agency EHRS IH module shall be used to the maximum extent possible for OCHMO-defined IH requirements, including exposure characterizations, records retention (e.g., ergonomics evaluation, exposure or incident investigations, Indoor Air Quality (IAQ) surveys, and EH instrumentation inventory records).
4.1.4 Center Policies and Procedures
4.1.4.1 Centers shall have all the appropriate Center-level policy level documents, as required by EH applicable regulations and this NPR.
4.1.4.2 Centers shall develop and maintain procedural level documentation to adequately and consistently implement their programs.
4.1.5 Emergency Preparedness
4.1.5.1 The OCHMO shall provide guidance and advice to NASA Centers on EH emergency preparedness.
4.1.5.2 The Director of Health and Medical Systems shall ensure Center EH emergency preparedness policy and programs are assessed for efficacy through regular, periodic reviews.
4.1.5.3 EH organizations shall develop emergency management plans to implement their roles and responsibilities as specified in their respective Center Emergency Management Plans.
4.1.5.4 Center EH organizations shall participate, at least annually, in Center emergency drills and lessons learned.
4.1.5.5 EH organizations shall use lessons learned to improve EH emergency responses.
4.1.6 Notification Requirements.
4.1.6.1 In addition to the reporting requirements specified elsewhere in this NPR, Centers shall inform the DASHO or Director of Health and Medical Systems, and the Senior Environmental Health Officer (SEHO), by the most expeditious means, of the following Center events:
a. Work-related death or in-patient hospitalization;
b. Official visits by any Federal, state, or local safety or EH regulatory agency;
c. Refusal of entry of any Federal, state, or local safety or EH regulatory agency;
d. Receipt of Federal, state, or local safety or EH regulatory citations;
e. Health and safety-related reports of reprisal or discrimination;
f. Reports of Immediately Dangerous to Life and Health (IDLH) working conditions;
g. Health and safety-related warrants/subpoenas; and
h. Other EH-related contact with any Federal or state agency or organization involving regulatory issues or agency-related agreements.
4.1.6.2 Centers shall inform the DASHO and OSMA, within 10 days, of the results of OSHA inspections and investigative reports of OSHA reportable events.
4.1.6.3 Centers shall inform the DASHO and OSMA, within 10 days, of corrective action reports or OSHA reportable events, replies to OSHA inspections, and reports of unsafe working conditions that are unresolved in 30 days.
4.1.6.4 Centers shall inform the SEHO of any and all coordination, partnering, collaboration, and other such agreements with Federal agencies within 10 days of first contact.
4.1.7 Training and Certification
4.1.7.1 All workers shall be effectively and adequately trained for the tasks they perform and shall meet at least the minimum applicable regulatory requirements for training and certification.
4.1.7.2 The requirements of OSHA Publication, OSHA 2254, Training Requirements in OSHA Standards, and Training Guidelines shall be met.
4.1.7.3 In addition to the safety training requirements required in 29 CFR 1960, 29 CFR 1910, and 29 CFR 1926, safety and health inspectors, managers, supervisors, safety and health specialists, safety and health committee members, and employees shall meet the requirements of NPR 8715.1, NASA Occupational Safety and Health Programs.
4.1.8 EH Budget and Resources
4.1.8.1 The NASA Administrator shall ensure that the Agency budget submission includes appropriate financial and other resources to effectively implement and administer the Agency's EH program per 29 CFR 1960.7, Financial Management.
4.1.8.2 The DASHO, Center Directors, Senior Center Managers, enterprise Program Managers, and OH CORs shall be responsible for planning, requesting resources, implementing, and evaluating EH program budgets in accordance with 29 CFR 1960.7(b), OMB Circular A-11 (sections 13.2(f) and 13.5(f), and other relevant documents).
4.1.8.3 The OCHMO shall provide guidance and advice to NASA Centers on the EH budget and resources.
4.1.8.4 The Director of Health and Medical Systems shall ensure Center EH budget and resources are assessed for efficacy through regular, periodic reviews.
4.1.8.5 Resources for EH programs shall include, but not be limited to, the following:
a. Sufficient personnel to implement and administer the program at all levels, including necessary administrative costs such as training, travel, and PPE;
b. Abatement of unsafe or unhealthful working conditions related to Agency operations or infrastructure;
c. Safety and health sampling, testing, and diagnostic and analytical tools and equipment, including laboratory analyses;
d. Capability to identify, analyze, and evaluate unsafe and unhealthful working conditions and operations;
e. Educational promotional costs such as publications, posters, or films;
f. Technical information, documents, books, standards, codes, periodicals, and publications;
g. Medical surveillance programs for personnel; and
h. Personnel, equipment, and other resources needed in support of the Agency Electronic Health Record System Industrial Hygiene module.
4.2.1 General
4.2.1.1 Unless specified elsewhere in this chapter, NASA Centers shall utilize OSHA Permissible Exposure Limits (PEL's), Threshold Limit Values (TLV's) issued by the American Conference of Governmental Industrial Hygienists (ACGIH) or specific NASA Health Standards issued by the OCHMO, whichever is more protective or whichever is selected by a competent person (See Appendix A).
Note: While the OSHA PEL's carry the weight of law, the majority of these regulations were adopted in 1970 from 1968 consensus values and most often do not reflect current scientific data. Additionally, there are currently only PEL's established for approximately 400 chemicals, which is a relatively small percentage of the thousands of chemicals that exist. For these reasons, NASA adopts the use of OEL's as a necessary and prudent practice.
4.2.2 Responsibilities
4.2.2.1 The OCHMO shall provide guidance and advice to NASA Centers on OELs.
4.2.2.2 The Director of Health and Medical Systems shall ensure Center OEL policy and programs are assessed for efficacy through regular, periodic reviews.
4.2.2.3 At a minimum, Centers shall follow the OEL's required by law, recommended and established by acknowledged authorities, and those developed specifically by NASA and shall apply whichever is more protective in the judgment of a competent person, such as a Certified Industrial Hygienist (CIH).
4.2.2.4 Centers shall be responsible for monitoring the workplace and workforce, selecting the most appropriate and protective OEL's for the work being performed, and ensuring people with appropriate training implement OEL's.
4.2.2.5 Centers shall be responsible for developing OEL's in the absence of an existing OEL for a specific chemical.
4.2.3 Process Description
4.2.3.1 In the absence of a specific PEL, TLV, or NASA Standard, other sources of OEL's shall be utilized. These include the following: (1) The National Institute for Occupational Safety & Health's (NIOSH) Recommended Exposure Limits (REL's); (2) The American National Standards Institute (ANSI) Standards; (3) The National Academy of Science Recommendations; (4) The American Industrial Hygiene Association (AIHA) Workplace Environmental Exposure Levels (WEELs); (5) The Environmental Protection Agency (EPA) Recommendations; (6) The Deutsche Forschungsgemeinschaft (German Commission for the Investigation of Health Hazards of Chemical Compounds in the Work Area) Maximum Allowable Concentrations; (7) The British Health & Safety Commission and Health & Safety Executive Occupational Exposure Limits and (8) Chemical manufacturers' recommended exposure values.
NOTE: When no established OEL exists for a specific chemical, a working OEL should be established by a competent person based on a thorough examination of the data available for that chemical and by following established industrial hygiene exposure limit setting guidelines. The process of establishing a working OEL should take into account chemical analogy, animal experimentation and extrapolation, and human experience and epidemiological data. In lieu of establishing a working OEL, Centers may take the approach of using control banding until an OEL is set by one of the organizations listed above. If Centers need assistance in determining OEL's, the Agency will pursue individual requests with the appropriate Federal agency or standard-setting organization.
4.2.3.2 Document the rationale used in establishing an OEL. The rationale should consider, summarize, and weigh the importance of all data. Additionally, experience and professional judgment shall be applied to weigh all information and apply an appropriate safety factor, based on the strength of the available data, before an OEL is established.
4.2.3.3 All of the available data used to establish the OEL shall be thoroughly documented.
4.2.3.4 Centers shall notify the OCHMO of all newly established OELs.
4.3.1 General
4.3.1.1 NASA Centers shall use a systematic and comprehensive approach to exposure assessment to anticipate, recognize, evaluate, and control health hazards in the workplace to effectively and proactively manage all EH programs.
4.3.2 Responsibilities
4.3.2.1 The OCHMO shall provide guidance and advice to NASA Centers on occupational exposure assessment and management.
4.3.2.2 The Director of Health and Medical Systems shall ensure Center occupational exposure assessment and management policy and programs are assessed for efficacy through regular, periodic reviews.
4.3.2.3 Centers shall employ a systematic and comprehensive approach to exposure assessment, establishing and implementing effective exposure assessment and management programs to anticipate, recognize, evaluate, and control health hazards in the workplace.
4.3.3 Process Description
4.3.3.1 EH programs shall establish a written Occupational Exposure Assessment and Management Program whose purpose is to collect and organize available information on the workplace; the workforce; chemical, physical, and biological agents; existing exposure controls; historical exposure data; biological monitoring data; and any other available source of information such as OEL's.
4.3.3.2 The written program shall include program goals and objectives and shall include an initial comprehensive exposure assessment, which shall be maintained current.
4.3.3.3 The outcome of this exposure assessment effort shall be a complete summary of available, essential information on workers, tasks, chemical, physical and biological agents, potential exposures (factoring in frequency and duration) and potential health effects.
4.3.3.4 Center EH programs shall create similar exposure groups (SEG's) and define exposure profiles for all identified exposure groups. The exception to this requirement would be research and test operations, which do not lend themselves to having similar exposures.
4.3.3.5 A determination shall be made about the acceptability, unacceptability, or uncertainty of the exposure profile defined for each SEG. Uncertain exposures shall lead to further information gathering. Unacceptable exposures shall lead to control of the exposure. Acceptable exposures shall lead to a periodic programmed reassessment based on risk.
4.3.3.6 Exposure groups with unacceptable exposures shall be prioritized and a strategy developed for exposure control.
4.3.3.7 OM clinics shall be notified regarding action level and unacceptable exposures for medical surveillance purposes and to identify SEGs.
4.3.3.8 Exposure assessment programs shall have a component that involves continual information gathering for the purpose of setting priorities on exposure groups for additional characterization and further information gathering. This can be either qualitative or quantitative information and shall be used to enhance the basic characterization and better define exposure groups, their profile, and the risks posed by exposure profiles.
4.3.3.9 Engineering controls shall be applied first. Until engineering controls are implemented or when engineering controls are not feasible, administrative controls or PPE shall be used. PPE shall be used as a last control measure.
4.3.3.10 Exposures shall be periodically re-characterized and reassessed in order to update exposure groups and exposure profiles.
4.3.3.11 The following records shall be maintained in accordance with NASA's record requirements and this NPR:
a. Lists of SEG's;
b. Exposure profiles; and
c. Judgments of acceptability.
4.4.1 General
4.4.1.1 The integrity of critical data shall be ensured by adherence to OSHA, NIOSH, or other recognized sampling and analytical methods using properly calibrated equipment with the National Institute of Standards and Technology (NIST) traceability, where applicable.
4.4.2 Responsibilities
4.4.2.1 The OCHMO shall provide guidance and advice to NASA Centers on sampling, analytical methods, and equipment calibration.
4.4.2.2 The Director of Health and Medical Systems shall ensure Center sampling, analytical methods, and equipment calibration policy and programs are assessed for efficacy through regular, periodic reviews.
4.4.2.3 Centers shall develop policies and procedures to ensure that proper sampling techniques, analytical methods, and equipment calibration are used throughout the data collection process.
4.4.2.4 Centers shall ensure adherence to OSHA, NIOSH, or other recognized sampling and analytical methods and use properly calibrated equipment with the NIST traceability, where applicable.
4.4.3 Process Description
4.4.3.1 Centers shall develop written policies and procedures for sampling, analytical methods, and equipment calibration utilizing methods established by professional or regulatory bodies. At a minimum, these requirements shall address sample planning, sampling methodology, pre-survey calibration, survey performance, sample collection, post-survey calibration, sample documentation, shipment of sample media, equipment calibration and maintenance, and recordkeeping.
4.4.3.2 Engineering, administrative, and PPE controls, in hierarchical order, shall be applied as appropriate whenever the sample exceeds the applicable OEL. Engineering controls shall be applied first. Until engineering controls are implemented or when engineering controls are not feasible, administrative controls or PPE shall be used. PPE shall be used as a last control measure.
4.4.3.3 Results shall be maintained in accordance with NASA recordkeeping requirements.
4.5.1 General
4.5.1.1 NASA Centers shall protect the reproductive health of the workforce and others from exposures to hazardous materials and articles (chemical, biological, radiological, and physical) that are known or suspected of being capable of posing a hazard to human reproduction.
4.5.1.2 Potential reproductive and developmental hazards shall be identified, and appropriate exposure control measures shall be implemented.
4.5.1.3 Exposures shall be kept As Low as Reasonably Practicable (ALARP) since short-term exposures to reproductive hazards can result in long-term health effects, and a developing fetus may also be adversely affected by exposures lower than those generally considered safe for adults.
4.5.2 Responsibilities
4.5.2.1 The OCHMO shall provide guidance and advice to NASA Centers on reproductive and developmental health.
4.5.2.2 The Director of Health and Medical Systems shall ensure Center reproductive and developmental health policy and programs are assessed for efficacy through regular, periodic reviews.
4.5.2.3 Centers shall develop, implement, administer, and maintain written Developmental and Reproductive Health Protection Programs that are designed to ensure the workforce and their unborn children are adequately protected from recognized hazards.
4.5.3 Process Description
4.5.3.1 Written developmental and reproductive health protection guidelines shall include provisions for:
a. Evaluating areas where potential chemical, biological, or physical reproductive hazards exist;
b. Determining the extent of potential exposures;
c. Developing/implementing procedures to reduce workplace exposures to reproductive hazards (i.e., engineering controls, job rotation, use of PPE, etc.);
d. Providing information and training on the chemical, physical, and biological hazards that may be present in the work area which may be reproductive and developmental health hazards;
e. Providing training on the proper use of PPE, safety devices, and other methods of decreasing exposure, including information on the declaration of pregnancy for radiological issues.
f. Implementing measures (for declared pregnancies) to achieve the lower exposure limit (0.5 rem to embryo/fetus during entire gestation period) and conducting dose monitoring;
g. Managing written declaration of pregnancies for workers exposed to radiological hazards.
NOTE: See sections entitled Radioactive Materials and Ionizing Radiation-Generation Equipment of this Chapter for more information.
h. Ensuring that known reproductive hazards specific to a work area are described in a written Job Safety Analysis (JSA), Job Hazard Analysis (JHA), or other hazard documentation.
i. Ensuring that supervisors provide individual operational training to assure reduced risk of exposures;
j. Maximizing worker privacy when implementing the elements of the program;
k. Notifying Center OM clinics of areas with potential exposures for medical surveillance purposes.
l. Notifying EH regarding new areas that may require workplace hazard assessment;
m. Ensuring that alternate job duties are considered when indicated by the OM clinic;
n. Designating the person responsible for arranging reasonable accommodations, if available; and
o. Designating the person responsible for counseling the affected person about other options, including sick leave and family leave when a reasonable accommodation is not available.
4.5.3.2 Center EH organizations shall perform additional workplace hazard assessments upon the request or when changes occur to ensure existing controls (engineering, administrative, and PPE) are adequate to protect workers from reproductive hazards.
4.5.3.3 The additional workplace hazard assessment shall include:
a. Identification of chemical, biological, physical, and radioactive agents in the workplace that present a potential exposure risk;
b. A qualitative exposure assessment of the concerned worker;
c. A review of work practices and PPE used, and recommendations for additional control measures, if needed; and
d. A review of past EH reports and historical sampling results, if available.
4.6.1 General
4.6.1.1 Nanomaterial, as currently defined by NIOSH, may pose an unusual risk to human health due to their unique composition, reactivity, size, and ability to cross cell membranes. All work with manufactured nanomaterial shall be prudently conducted in a manner that is responsible and safe.
4.6.2 Responsibilities
4.6.2.1 The 4.6.2.1 OCHMO shall provide guidance and advice to NASA Centers on nanotechnology.
4.6.2.2 The Director of Health and Medical Systems shall ensure Center nanotechnology policy and programs are assessed for efficacy through regular, periodic reviews.
4.6.2.3 Centers shall ensure that all work with manufactured nanomaterial adheres to NASA's requirements as per 4.6.1.1 of this document.
4.6.2.4 Centers with nanomaterial shall have written nanotoxicology programs that are designed and implemented to ensure all work with manufactured nanomaterial minimizes exposures to an ALARP level, or to other exposure standards as described in this NPR.
4.6.3 Process Description
4.6.3.1 Center nanotoxicology programs shall encompass the requirements of this section.
4.6.3.2 Transportation, storage, use, and disposal of manufactured nanomaterial shall be conducted in accordance with all Federal, state, local, Agency, and Center requirements.
4.6.3.3 Workers potentially exposed to manufactured nanomaterials shall be informed of the risks associated through training programs, safety data sheets, labeling, and signage.
4.6.3.4 Centers shall conform to best available work practices, such as, but not limited to, those from NIOSH, OSHA, or FDA for products that utilize nanotechnology and/or contain manufactured nanomaterial.
4.6.3.5 Centers shall conduct Hazard Assessments (HA's) prior to beginning work with manufactured nanomaterial.
4.6.3.6 HA's shall be conducted by a competent person who shall identify appropriate engineering controls, administrative controls, and personal protective equipment to ensure worker safety.
NOTE: A competent person is a person who has acquired through training, qualification, and experience, the knowledge, skills, and professional judgment to identify hazardous materials and/or articles and who has the designated ability to manage those substances and/or articles that are brought onto the Center. This is generally an American Board of Industrial Hygiene (ABIH) CIH.
4.6.3.7 HA's shall evaluate several factors, including, but not limited to, the physical and chemical properties of the nanomaterial, the process by which it will be generated and/or used, and the adequacy of existing engineering controls (e.g., fume hood, glove box).
NOTE: In some instances, the competent person may recommend collecting occupational exposure measurements (e.g., sampling) to further understand potential hazards or to identify specific processes or equipment requiring additional engineering controls.
4.6.3.8 Exposures to manufactured nanomaterial shall be kept to a minimum ALARP by utilizing the basic hierarchy of controls described below, as prescribed by a competent person with the exception of a material being in solution or embedded in substrate where it cannot become airborne.
NOTE: Although traditional OEL's exist for many of the materials from which nanomaterial is made, the OEL for a nanomaterial of these substances is not yet clear. As a result, NASA approach for controlling exposures to nanomaterial differs from those of traditional hazardous materials covered in the section entitled Occupational Exposure Assessment and Management.
a. Engineering. These controls may include local exhaust ventilation and localized filtration.
b. Administrative. It is important to incorporate administrative controls, such as scheduling maintenance of fume hoods on off hours, and limiting potential exposure time, into operations involving nanomaterial's due to the ambiguity about nanomaterial OELs. The incorporation of good work practices helps to minimize exposure to manufactured nanoparticles.
c. PPE. Typical chemistry laboratory apparel and PPE shall be worn when working with manufactured nanomaterial. This includes long pants, shirts, and shoes, as well as safety glasses, laboratory coats, gloves, and eye protection. If the nanomaterial can become airborne (not in solution or embedded in substrate), then respiratory protection is required. Open sandals, shorts, and skirts are prohibited. Respiratory protection shall be utilized when local exhaust ventilation and filtration are not available or feasible for work involving manufactured nanomaterial not suspended in liquids or embedded in substrate. However, the preferred method for manipulating manufactured nanomaterial is in solution, and every effort should be made to design and implement effective engineering controls for any operation where manufactured nanomaterial are used.
4.6.3.9 Spill management shall be addressed emphasizing that all debris resulting from the cleanup of a manufactured nanomaterial spill shall be handled as though it were hazardous and include procedures for access control and cleanup of both dry and wet materials.
4.7.1 General
4.7.1.1 NASA Centers shall evaluate the potential exposure issues involved with the use of hazardous materials and articles.
4.7.1.2 Hazardous materials and/or articles shall not be procured or otherwise acquired until hazards have been analyzed and adequate controls selected.
4.7.1.3 Hazardous materials and/or articles shall not be brought onto Centers until adequate controls have been implemented.
4.7.2 Responsibilities
4.7.2.1 The OCHMO shall provide guidance and advice to NASA Centers on hazardous materials and articles acquisitions.
4.7.2.2 The Director of Health and Medical Systems shall ensure Center hazardous materials and articles acquisition policy and programs are assessed for efficacy through regular, periodic reviews.
4.7.2.3 NASA Centers shall be responsible for:
a. Administering and identifying hazardous material and article acquisitions;
b. Maintaining and monitoring the effectiveness of hazardous material and/or article acquisition programs, including all mechanisms for acquiring hazardous materials and articles;
c. Reviewing the records of purchases, at least annually, to ensure that hazardous materials and/or articles acquisitions are being properly reviewed and approved by competent persons and occupational health safety requirements are being properly implemented prior to acquisition;
d. At a minimum, following the manufacturer's product recommendations and requirements, except when directed by a competent person to use alternate controls or where inconsistent with the requirements of Section 4.8 or generally accepted practices;
e. Monitoring conformance with the requirements and reporting nonconformances to Center or Facility Managers; and
f. Ensuring the requirements of this section are included in all contract procurements with provisions to extend the requirements into subcontracts.
4.7.2.4 Competent Persons shall review procurements and other acquisitions of hazardous materials and/or articles, and coordinate with Center occupational safety and health organizations to:
a. Identify hazards associated with the materials and/or articles being obtained;
b. Identify alternatives, where available, to reduce risk;
c. Determine safety and health requirements for the safe use of hazardous materials and/or articles; and
d. Disapprove acquisitions of hazardous materials and/or articles that cannot be safely used.
4.7.3 Process Description
4.7.3.1 Each Center shall implement a means to control and regulate acquisitions of hazardous materials and/or articles.
4.7.3.2 Each Center shall implement a means to hold purchasers and receivers accountable for the proper and safe acquisition of hazardous materials and articles.
4.7.3.3 The following requirements shall be implemented prior to hazardous materials and/or articles acquisition:
a. Use of less hazardous materials or articles, if materials and/or articles can reasonably be substituted;
b. Acquisition of the smallest reasonable amount, size, activity, and/or hazard potential;
c. Approval of the acquisition by an Competent Person; and
d. Completion of hazard determinations, training, and other pertinent preparations adequate to ensure safe use.
4.8.1 General
4.8.1.1 NASA Centers shall protect and conserve the hearing of the workforce from occupational exposures to hazardous noise by identifying hazardous noise areas and appropriately implementing noise exposure control measures.
4.8.1.2 Any work area where the environmental noise level is at or above 85 dB A-weighted (dBA), or where the environmental impulse noise level is at or above 140 dB peak C-weighted (dBC) or linear, regardless of duration of exposure or number of impulses, shall constitute a hazardous noise area.
4.8.1.3 This section outlines additional requirements to those established in 29 CFR 1910.95, Occupational Noise Exposure Hearing Conservation Amendment Final Rule and appendices and 29 CFR 1904.10, Occupational Injury and Illness Recordkeeping and Reporting Requirements for prevention of noise-induced hearing loss where workers are occupationally exposed to hazardous noise. It applies to all NASA occupational settings except space flight.
4.8.1.4 The implementation of a written site-specific Hearing Conservation Program (HCP) shall be the mandatory means by which Centers and other field facilities apply Federal, state, local and NASA Hearing Conservation standards and associated program requirements. In addition, Centers shall administer a continuing, effective HCP in conformance with the requirements of this section with all the affected workers included in the program.
4.8.1.5 Personnel knowledgeable in sound analysis, noise exposure assessment, hearing protection, audiometric testing, and noise abatement strategies shall implement HCP and associated programs.
4.8.1.6 Center's HCP self-reviews shall be documented and performed at least annually. A self-review shall consist of items such as, but not limited to, review of Standard Threshold Shift (STS), review of hazardous noise areas, and review of monitoring equipment.
4.8.1.7 Site-specific "Buy Quiet" and "Quiet by Design" programs shall be implemented to protect workers and assure that purchases and designs are best values (i.e., having lowest, long-term cost of exposure to noise produced by the purchase of equipment) and in NASA's best interest.
4.8.1.8 Workers exposed to noise equal to or exceeding the NASA action level of 82 dBA Time-weighted Average (TWA) for 30 days or more per year, or those who can be expected to be exposed to 85 dBA TWA for any one day, shall be enrolled in a HCP that meets the requirements of this NPR. Exposures shall be computed without regard to any attenuation provided by the use of personal protective equipment.
NOTE: NASA's Action Level for noise is the equivalent to an 82 dBA, 8-hour TWA exposure, using a 3 dB exchange rate, as shown in Table 1 Below.
NASA's Action Level Equivalent Exposures: Table 1
| Level (dBA) | Hour | Minutes | Seconds |
|---|---|---|---|
| 79 | 16 | 0 | 0 |
| 80 | 12 | 41 | 57 |
| 81 | 10 | 4 | 46 |
| 82 | 8 | 0 | 0 |
| 83 | 6 | 20 | 59 |
| 84 | 5 | 2 | 23 |
| 85 | 4 | 0 | 0 |
| 86 | 3 | 10 | 29 |
| 87 | 2 | 31 | 11 |
| 88 | 2 | 0 | 0 |
| 89 | 1 | 35 | 15 |
| 90 | 1 | 15 | 36 |
| 91 | 1 | 0 | 0 |
| 93 | 0 | 37 | 48 |
| 94 | 0 | 30 | 0 |
| 95 | 0 | 23 | 40 |
| 96 | 0 | 18 | 54 |
| 97 | 0 | 15 | 0 |
| 92 | 0 | 47 | 37 |
4.8.1.9 Workers who enter designated areas or who perform tasks where exposure to noise is greater than or equal to 82 dBA, regardless of the duration of exposure, shall be provided with personal Hearing Protection Devices (HPDs).
4.8.1.10 Workers who enter designated hazardous noise areas or who perform tasks where exposure to noise is greater than or equal to 85 dBA or 140 peak dBC or linear, regardless of the duration of exposure or number of impulses, shall be provided with and required to wear personal HPDs.
4.8.1.11 NASA's noise exposure limit (Criterion Sound Level) is the equivalent to an 85 dBA, 8-hour TWA exposure using a 3 dB exchange rate as shown in Table 2 below.
Noise Exposure Limits (Equivalent Exposures): Table 2
| Level (dBA) | Hours | Minutes | Seconds |
|---|---|---|---|
| 81 | 20 | 10 | 0 |
| 82 | 16 | 0 | 0 |
| 83 | 12 | 42 | 0 |
| 84 | 10 | 5 | 0 |
| 85 | 8 | 0 | 0 |
| 86 | 6 | 21 | 0 |
| 87 | 5 | 2 | 0 |
| 88 | 4 | 0 | 0 |
| 89 | 3 | 10 | 0 |
| 90 | 2 | 31 | 0 |
| 91 | 2 | 0 | 0 |
| 92 | 1 | 35 | 0 |
| 93 | 1 | 16 | 0 |
| 94 | 1 | 0 | 0 |
| 95 | 0 | 47 | 37 |
| 96 | 0 | 37 | 48 |
| 97 | 0 | 30 | 0 |
| 98 | 0 | 23 | 49 |
| 99 | 0 | 18 | 59 |
| 100 | 0 | 15 | 0 |
NOTE: Table 2 contains noise exposure levels and durations that are equivalent to this limit as calculated by the following formula where L stands for exposure level and T for duration: T (min) = 480/2 (L-85)/3. Noise dose shall include all impact/impulse noise measured up to and including 140 peak dBC or linear.
4.8.1.12 The definitions in 29 CFR 1910.95, Occupational Noise Exposure, Appendix I, are applicable to this section unless otherwise defined in Appendix A of this NPR.
4.8.1.13 Exposures exceeding the limits in Table 2 shall be controlled, reduced, or eliminated through a hierarchical combination of engineering controls, administrative controls, and hearing protection devices.
4.8.1.14 Engineering controls shall be the first and primary means of controlling hazardous noise.
4.8.2 Responsibilities
4.8.2.1 The OCHMO shall provide guidance and advice to NASA Centers on hearing conservation.
4.8.2.2 The Director of Health and Medical Systems shall ensure Center hearing conservation policy and programs are assessed for efficacy through regular, periodic reviews.
4.8.2.3 Centers shall implement written HCP Programs.
4.8.2.4 The Agency Chief Engineer and the Agency Assistant Administrator of Strategic Infrastructure shall ensure that "Buy Quiet and Quiet by Design" provisions are integral to site selection and the design of new or modified facilities and equipment.
4.8.2.5 The Agency Assistant Administrator for Procurement shall ensure that "Buy Quiet" and "Quiet by Design" provisions are included in contracts and in the purchase of new equipment that generates 80 dBA or greater at 3 feet.
4.8.2.6 Center Directors and the Assistant Administrator for Strategic Infrastructure shall ensure that adequate facility resources are provided to implement Center HCPs, Buy Quiet Programs, and Quiet by Design Programs.
4.8.2.7 Center Purchase Requesters/Requirements Initiators shall coordinate with Center OH offices to ensure requirements documents include provisions for written HCPs, Buy Quiet Programs, and Quiet by Design Programs.
4.8.2.8 Contracting Officers shall work with Center OH officers and Purchase Requesters/Requirements Initiators to ensure that Center contract requirements include provisions for written HCPs, Buy Quiet Programs, and Quiet by Design Programs.
4.8.2.9 Medical Directors shall ensure that medical examinations relative to occupational noise are properly performed, appropriate records are maintained, and that all examination results are communicated to the affected person as specified in this NPR.
4.8.3 Process Description
4.8.3.1 Center HCPs shall include provisions for:
a. Specifying the individual responsibilities of Facilities Managers, Design Engineers, Occupational Health Personnel, Supervisors, and affected workers;
b. Assuring that noisy areas are surveyed to determine if they are hazardous noise areas and effectively prioritize noise surveys and noise remediation efforts;
c. Affirming the action level, criterion level, sound level, and exchange rate;
d. Evaluating and maintaining the HCP's effectiveness;
e. Implementing "Buy Quiet" and "Quiet by Design" Programs;
f. Performing and recording exposure monitoring and evaluating results;
g. Requiring effective intra-Center communication and coordination of Center disciplines to identify, evaluate, and control hazardous noise exposures;
h. Performing medical surveillance, including audiometric testing, review, and medical follow-up;
i. Notifying and coordinating information (noise exposure and dosimetry monitoring and survey results, operational and design plan review results, the addition of new equipment or new operations, and any work-related STS) among workers, management, and occupational health personnel;
j. Selecting, using, cleaning, and inspecting hearing protectors;
k. Training workers and supervisors of workers who are enrolled in a HCP;
l. Ensuring the Council for Accreditation of Occupational Hearing Conservation (CAOHC) certification of personnel performing audiometric testing. CAOHC certification is encouraged for nurse practitioners, physician assistants, and physicians. Professional Supervisor of Hearing Conservation is recommended for physicians evaluating work-relatedness of hearing loss;
m. Recordkeeping and accessing information in accordance with NASA's record requirements and this NPR;
n. Defining noise control requirements and strategies;
o. Effectively implementing engineering, operational, and administrative controls; and
p. Defining appropriate corrective actions for personnel and organizations that violate requirements of this section, the Center's HCP requirements, or 29 CFR 1910.95, "Occupational Noise Exposure Hearing Conservation Amendment Final Rule," and appendices.
4.8.3.2 "Buy Quiet and Quiet by Design" Programs shall:
a. Evaluate new equipment and systems to ensure they meet realistic and achievable noise emission criteria;
b. Encompass design, development, selection, and purchase of stationary and portable equipment purchased for use by Centers, including equipment purchased by contractors to minimize noise exposure hazards to workers;
c. Include all equipment expected to produce noise approaching hearing conservation levels of 80 dBA and higher;
d. Identify noise emission and control requirements for equipment procurement, specifications, and design;
e. Contain provisions for program support, promotion, training, and management sponsorship;
f. Be individualized to meet Center-specific needs, configuration, and other relevant factors;
g. Incorporate and follow the "Buy Quiet Roadmap" for all covered procurements. Centers are permitted to utilize an alternative formal process that provides equivalent documentation of key decisions, authorizations, and verifications.
4.8.3.3 Engineering Controls shall:
a. Be the first and primary means of controlling hazardous noise. The feasibility and cost of engineering controls may be considered when making decisions about these controls;
b. Aim to reduce noise emissions (measured at operator position or equivalent) to below 85 dBA; and
c. Be reviewed at least annually to assess the adequacy of precautions that are planned and/or implemented to control noise exposures.
4.8.3.4 Engineering projects shall include noise control measures and operational plans that have been previously coordinated with and approved by affected Center management organizations and occupational health personnel. Coordination shall be done in the early stages of the design and/or planning process, prior to contract award, and/or before "authority to proceed."
4.8.3.5 Organizations responsible for introducing changes to facilities, operations, or procedures shall notify Center occupational health personnel of:
a. Changes in operations or equipment that increases noise levels; and
b. New, uncontrolled, or previously unidentified areas, operations, or equipment that may produce hazardous noise or may not comply with the requirements of this section.
4.8.3.6 If engineering controls fail to reduce sound levels to the requirements specified in this section, administrative controls shall be utilized. Examples of administrative controls include access restrictions and time limitations in the hazardous noise area. Specific requirements for administrative controls include maximizing the distance between the person and the hazardous noise source to the extent practical; and appropriately identifying hazardous noise areas.
4.8.3.7 If engineering and administrative controls fail to reduce sound levels to within the requirements specified in this section, exposures shall be brought to acceptable levels by using Hearing Protection Devices (HPDs).
4.8.3.8 Centers shall be responsible for identifying hazardous noise areas and hazardous noise producing equipment according to the following criteria:
a. Signs shall clearly indicate the presence of hazardous noise and state the requirement to wear hearing protection.
b. The signs shall be posted at the entrance(s) to or the periphery of hazardous noise area(s).
c. Power tools and machines that produce hazardous noise levels shall be labeled using decals, placards, or other signage with similar statements, and warning signs shall be posted in areas where hazardous noise-producing tools and machines are used.
4.8.3.9 Disposable HPDs shall be for the exclusive use of each person and shall not be traded or shared. Non-disposable HPDs shall be properly sanitized and inspected prior to use by another person.
4.8.3.10 HPDs shall attenuate noise exposure to an 8-hour, TWA of 85 dBA or less. For those persons with an STS, HPDs shall attenuate exposure to an 8-hour, TWA of 82 dBA or less. The published Noise Reduction Rating (NRR) value may be used, if available. When using de-rating criteria for each noise area, HPD attenuation shall be determined by the most conservative method for defining the NRR of HPDs.
4.8.3.11 The adequacy of HPD attenuation shall be re-evaluated whenever workers noise exposures increase.
4.8.3.12. Special hearing-protective equipment, such as sound-suppression or noise-cancellation communication headsets, shall be regularly inspected if they are used in hazardous noise areas.
4.8.3.13 Sound-suppression and noise-cancellation headsets that have been damaged, altered, or modified in any way that affect the attenuation characteristics shall not be used.
4.8.3.14 Where sound-suppression and noise-cancellation headsets are not permanently issued to individuals, such equipment shall be cleaned and sanitized before re-issuance.
4.8.3.15 Noisy areas shall be surveyed to determine if they are hazardous noise areas in accordance with the following requirements:
a. Measurement of potentially hazardous sound levels shall be conducted when any information, observation, or calculation indicates that a person may be exposed to noise at or above the action level (50 percent of the OEL). This includes, but is not limited to, times where there is a need to document representative noise exposures, where workers complain of excessive noise, or where it is difficult to understand a normal conversation when the speaker and listener face each other at a distance of 3 feet;
b. Noise surveys shall also be conducted whenever any changes to facilities, equipment, work practices, procedures, or noise-control measures alter potential noise exposures. A review of hazardous noise sources and controls, worker exposures, and work practices and procedures shall be conducted for changed conditions whenever a worker experiences an STS;
c. In determining TWA exposures, all continuous, intermittent, and impulsive sound levels shall be integrated into the noise measurements;
d. Octave band analysis shall be conducted, as necessary, to establish the characteristics of the noise source and to help determine appropriate abatement techniques;
e. When a noise survey is performed, it shall determine the presence of compounding hearing related circumstances present in the environment (e.g., certain solvents, heavy metals, carbon monoxide, heat, and vibration) to ensure proper mitigation;
f. Exposure monitoring shall be conducted when a noise survey shows that a worker/workers may be exposed to noise at or above 82 dBA, 8-hour TWA. The purpose of such monitoring is to determine the noise dose of the exposed worker(s), the representative exposure of similarly exposed workers, and, if warranted, the appropriate noise abatement techniques;
g. Operational plans shall be reviewed to assess the adequacy of precautions that are planned and/or implemented to control noise exposures;
h. Assessments shall be conducted of each operation, job, or procedure having the potential to create hazardous noise;
i. New equipment, operations, jobs, or procedures, with the potential for creating hazardous noise, shall be evaluated with regard to noise emissions prior to operational start up;
j. Workers and/or their representatives shall be provided an opportunity to observe noise dosimetry and area monitoring activities;
k. Affected workers shall be notified in writing of the results of noise dosimetry monitoring;
l. Employers of affected workers and their responsible occupational health program managers shall be notified when noise measurement data indicate that noise exposures equal or exceed the action level or the limitations of Table 1. Written reports of the hazardous noise surveys shall identify survey observations, findings, and conclusions and shall be provided to affected employees; and
m. Hazardous noise areas shall be identified, selected, and surveyed. A review of each hazardous noise area for changes in conditions, noise sources, and configuration shall be documented at least annually.
4.8.3.16 Instruments used to measure workers' noise exposures shall adhere to the following requirements:
a. Instruments shall be field-calibrated or calibrated to manufacture's specifications prior to use;
b. Instruments shall be checked and calibrated at least annually by the manufacturer, a representative of the manufacturer, or an approved laboratory; and
c. Sound-level meters used to measure worker noise exposures shall be set at "slow" response and A-weighting.
4.8.3.17 Audiometric test equipment shall be calibrated to meet the requirements specified in the latest revision of ANSI S3.6, Specification for Audiometers.
4.8.3.18 Ambient noise levels in audiometric test rooms and booths shall meet the specifications in the latest version of ANSI S3.1, Maximum Permissible Ambient Noise Levels for Audiometric Test Rooms.
4.8.3.19 Medical surveillance shall be provided to all workers enrolled in a HCP in accordance with the following requirements:
a. Workers receiving medical surveillance shall undergo a baseline audiometric examination before beginning work assignments in hazardous noise areas;
b. If it is not possible to obtain the baseline prior to noise assignment, then workers shall undergo a baseline audiometric examination within 30 days of initial exposure to hazardous noise. During this 30-day period, workers shall wear personal HPDs, which reduce their exposure to 82 dBA TWA or below. When it is discovered that workers have already been assigned to a position that may expose them to hazardous noise but have not yet had an audiometric examination:
(1) Audiometry shall be conducted within 30 days of the discovery, and workers shall wear personal hearing protection that reduces their exposure to 82 dBA TWA or below until audiometry has been conducted.
(2) A documented root cause analysis shall be made to determine the cause(s) of the oversight, and positive and affirmative action(s) taken to avoid recurrence.
c. Audiometric examinations shall include audiometry, an otoscopic examination by an audiologist, physician, or CAOHC certified Occupational Hearing Conservationist to identify any existing abnormal medical conditions of the ear, and an update to the person's medical record to document past noise exposure and other otopathological factors;
d. The person shall have no apparent or suspected ear, nose, or throat problems that might compromise the validity of the audiogram. When a person has an acute disease that may compromise the validity of the test, audiometry shall be delayed until the condition has abated;
e. The exposure and medical history taken at the time of the audiometric examination shall include ototoxic medications and exposure to ototoxic substances or materials;
f. Workers suffering from acute diseases of the ear shall not be placed in hazardous noise areas until the condition has abated, particularly if such diseases preclude the wearing of hearing protectors;
g. Centers shall take all reasonable measures to ensure that workers who have participated in the HCP medical surveillance program receive a final audiometric examination prior to termination of employment, transfer to duties not involving noise exposures, transfer to another installation, or retirement. An annual audiogram, if completed within six (6) months prior to termination, transfer, or retirement date, may serve as the final audiogram; and
h. When workers at a Center retain their "work role position" but change employers due to contract award to a new employer, all medical records applicable to hearing conservation shall follow them to their new employer, including their current baseline threshold.
4.8.3.20 Audiometric testing shall be performed upon initial assignment, and annually thereafter, in accordance with 29 CFR 1910.95, Sections (g) and (h) and additionally as follows:
a. Audiologists and/or physicians knowledgeable in hearing conservation shall oversee all audiometric testing conducted by CAOHC-certified Occupational Hearing Conservationists;
b. Personnel who conduct audiometric testing shall be familiar with the provisions of this section;
NOTE: An STS is defined as a decline in hearing threshold, relative to the baseline audiogram, of an average of 10 dB or more at 2000, 3000, and 4000 Hz in either ear.
c. All baseline audiograms and confirmation audiograms following the identification of an STS shall be preceded by a period of at least 14 hours during which there shall be no exposure to noise above 82 dBA TWA, on or off the job. Hearing protectors that lower workplace noise to the equivalent of 82 dBA TWA, using the appropriate noise-reduction rating, may be used to conform to this requirement;
d. If during any medical evaluation or audiometric examination the worker is identified as potentially unable to perform his or her job safely or has a hearing profile equal to or worse than that listed in Table 3 below, the worker and his or her employer shall receive a written notification of the requirement to perform a Functional Ability Evaluation. The written notification shall include results of pertinent work history and relevant conditions, e.g., visual impairment, that may affect ability to safely perform the work expected in the position held or to wear appropriate personal hearing protection equipment in a hazardous noise area.
Table 3
| Frequency (Hz) | 500 | 1000 | 2000 | 3000 | 4000 | 6000 |
| Hearing Threshold Level (dB) | 25 | 25 | 25 | 35 | 45 | 45 |
4.8.3.21 The requirements for handling threshold shifts are as follows:
a. The STS should be computed using the age corrections described in OSHA 29 CFR 1910.95, Appendix F;
b. Each employee's annual audiogram shall be compared to his/her baseline audiogram to determine if the audiogram is valid and to determine if an STS has occurred;
c. The baseline of each ear shall be separately tracked;
d. A physician, audiologist, or CAOHC-certified Occupational Hearing Conservationist shall perform the hearing test and make the comparison;
e. If an STS is identified and a confirmation audiogram is not obtained within 30 days, the STS shall become a confirmed STS by default;
f. If the identified STS is followed by a confirmation audiogram and the confirmation audiogram does not confirm the STS, this second audiogram replaces the first one;
g. If the identified STS is followed by a positive confirmation audiogram, the better of the two shall become the confirmed STS;
h. An audiologist or physician with hearing conservation experience shall review problem audiograms, including those showing an STS (either by confirmation within 30 days or by default) and shall determine whether there is a need for further evaluation.
i. When further evaluation is warranted, the worker shall be referred to an otolaryngologist or other qualified physician, or to an audiologist for further medical evaluation, and
j. A new baseline reference audiogram shall replace the original or previous baseline audiogram (in separate ears and not both ears, unless both ears meet criteria listed below) when:
(1) The reviewer determines that an STS is persistent on a retest (conducted no sooner than six (6) months later). Persons assigned a new baseline audiogram, as a result of an STS, shall receive an audiometric re-evaluation six (6) months after this assignment to determine if a further STS has occurred. The baseline shall be revised to the STS test which shows the lower (more sensitive) value for the average of thresholds at 2000, 3000, and 4000 Hz.
(2) A "significant improvement" is shown if the average of thresholds at 2000, 3000, and 4000 Hz for either ear shows an improvement of 5 dB or more from the baseline and the improvement is persistent in the next test. The baseline shall be revised to the improved test which shows the lower (more sensitive) value for the average of thresholds at 2000, 3000, and 4000 Hz. Age corrections shall not be used when determining "improvement."
(3) An audiologist or physician may determine that reasons exist for not revising an employee's baseline audiogram. In such cases, the audiologist or physician must document the reasons for not revising the baseline.
k. The worker, employer, and Center environmental health staff shall be notified of an STS in writing within 21 days of the determination of the STS;
l. If the worker's uncorrected hearing threshold level (HTL), without age correction (averaging 2000, 3000, and 4000 Hz) is 25 dB or greater above audiometric zero in the same ear as the STS, a work relatedness determination shall be made;
m. Based on the best available information, a physician or other licensed health care professional, in consultation with the employer, shall determine whether the noise-induced STS is work-related;
n. Unless a physician has determined that the STS is not work-related, the following actions shall be taken:
(1) The worker's management and responsible safety and health office shall be notified of the occurrence of an STS or other work-related hearing loss.
(2) The work-related hearing loss shall be relayed to the Center's mishap reporting system.
(3) The worker shall be notified and examined by a physician or an audiologist for proper HPD fit.
(4) HPDs shall be re-evaluated for effectiveness, and the worker shall be refitted, as necessary, with HPDs offering a greater sound attenuation.
(5) The worker shall be re-trained on the hazardous effects of noise and the need to use hearing protection.
(6) The work environment(s) shall be re-investigated to determine if work practices or changes in equipment or procedures have increased the noise hazard. Abatement actions shall be instituted, as necessary, with engineering controls employed as a first priority to reduce the potential for exposure to the action level.
(7) Any administrative and work practices being utilized to reduce noise exposures shall be reevaluated for effectiveness.
o. The Medical Director shall determine if reassignment to work in a low noise area is indicated to prevent further hearing impairment and shall advise the employer accordingly;
p. The employer shall have ultimate authority and responsibility for worker reassignment; and
q. Where the same worker experiences any subsequent work-related STS as a result of occupational noise exposure, the work environment(s) shall be re-evaluated. If the worker continues to work in the hazardous noise area(s), engineering and/or administrative controls shall be employed that reduce that worker's noise exposure to no more than 50 percent of what was previously allowed for that worker.
4.8.3.22 Unless a physician has determined a standard threshold shift is not work related or aggravated by occupational noise, the following steps shall be taken when an STS occurs:
a. Workers shall be referred to an otolaryngologist/physician knowledgeable in hearing conservation or to an audiologist for more comprehensive testing when it is suspected medical pathology of the ear is caused or aggravated by the wearing of hearing protectors;
b. Workers shall be informed of the need for an otological examination if a medical pathology of the ear unrelated to the use of hearing protectors is suspected; and
c. Workers shall be referred for persistent failure to obtain a valid audiogram.
4.8.3.22.1 To support the identification of larger changes in hearing that may be medically significant or result in communication difficulties, the following American Academy of Otolaryngology—Head and Neck Surgery occupational hearing referral criteria are recommended:
(1) An average HTL at 500, 1000, 2000, and 3000 Hz greater than 25 dB HTL in either ear (Baseline Audiogram).
(2) A difference in average HTL level between the better and poorer ears of more than 15 dB HTL at 500, 1000, and 2000 Hz (Baseline Audiogram).
(3) A change for the worse in average HTL in either ear compared to the baseline audiogram of more than 15 dB HTL at 500, 1000, and 2000 Hz or more than 20 dB HTL at 3000, 4000, and 6000 Hz (Periodic Audiograms).
(4) A history of ear pain; drainage; dizziness; severe, persistent tinnitus; sudden, fluctuating or rapidly progressive hearing loss; or a feeling of fullness or discomfort in one or both ears within the preceding 12 months (Any Audiogram).
(5) Earwax accumulation sufficient to completely obstruct the view of the eardrum during otoscopic examination or a foreign body is present in the ear canal.
4.8.3.23 The latest edition of the American Medical Association Guides to the Evaluation of Permanent Impairment shall be used as a guideline in determining hearing impairment.
4.8.3.24 All HCP and/or hazardous noise training shall be conducted based on the criteria of this section.
a. Each Occupational Hearing Conservationist shall receive CAOHC certification. A CAOHC refresher course shall be taken at least every five (5) years;
b. Occupational health personnel who conduct assessments shall receive initial training on their Center's hearing conservation program and in the hazards of noise exposure;
c. Workers and supervisors of workers enrolled in a HCPs shall receive annual training in the hazards of noise exposure; and
d. Annual training in the hazards of noise exposure shall include, at a minimum:
(1) An overview or review of the 29 CFR 1910.95, the Center's and employer's (if a contactor) HCP, and this section.
(2) The effects of hazardous noise and ototoxic substances or materials on hearing (including permanent hearing loss).
(3) Identification of the hazardous noise sources in the employee's work areas.
(4) Factors that may contribute to hearing loss.
(5) Noise-control principles.
(6) An explanation of the audiometric testing procedure and the purpose of audiometric testing.
(7) The employee's role and responsibilities in the HCP.
(8) The purpose of HPD's, including:
(a) The advantages, disadvantages, and attenuation characteristics of various types of HPD's;
(b) Instructions on selection, fit, use, and care of HPD's; and
(c) The recommendation that employees use hearing protection whenever there is exposure to hazardous noise during off-duty activities (e.g., lawn mowing, use of firearms).
4.8.3.25 Accurate HCP records shall be maintained as specified in the applicable records retention schedules in NPR 1441.1 and the Records Management Plan for the NASA Electronic Health Record System.
4.8.3.26 Records kept shall follow the requirements of NPR 1441.1, NASA Records Retention Schedules, and shall include, but are not limited to:
a. The Center's written HCP and subsequent revisions;
b. A comprehensive registry of all workers placed in the HCP;*
c. Audiometric tests and records;*
d. Background sound pressure levels of audiometric test rooms;
e. Data and information concerning repair of audiometers;
f. Hazardous noise area locations and noise levels recorded in those areas;
g. Survey and dosimetry results and recommendations;*
h. Data and information concerning calibration and repair of sound-measuring equipment;
i. The employee's most recent noise-exposure assessment;
j. Special noise studies;
k. Remedial actions recommended/taken;
l. Engineering controls installed;
m. Results of design and operational reviews;
n. Training; and
o. Hearing protector selection.
NOTE: Items above marked with an asterisk (*) shall be maintained for at least 30 years.
4.8.3.27 Documentation of other official HCP-related activities shall be as follows:
a. Audiometric test records shall include, as a minimum:
(1) Hearing threshold levels at 500, 1000, 2000, 3000, 4000, 6000, and 8000 Hz.
(2) The audiometric reference level to which the audiometer was calibrated at the time of testing.
(3) The date of the audiogram.
(4) The worker's first and last names, employee number, and job classification.
(5) The examiner's name and position.
(6) The date of the last calibration of the audiometer.
b. Audiograms and noise-exposure records shall be maintained as a permanent part of a worker's medical record;
c. When noise-exposure-measurement records are representative of the exposures of other individuals participating in the HCP and to the extent allowable by the Privacy Act and where applicable to the HIPAA, the range of noise levels and the average noise doses shall be made a permanent part of the medical records of those other individuals; and
d. Consistent with applicable requirements, copies of this section, 29 CFR 1910.95, and any other records required by this section, shall be provided upon written request to:
(1) Workers and former workers and their representatives.
(2) Representatives of the U.S. Department of Labor.
(3) The National Institute for Occupational Safety and Health (NIOSH).
(4) NASA Occupational Health Program personnel.
4.9.1 General
4.9.1.1 NASA Centers shall encourage participation in developing, implementing, and evaluating ergonomics programs.
4.9.1.2 Musculoskeletal Disease (MSD) signs and symptoms shall be evaluated in all areas where potential ergonomic hazards exist, and that ergonomic hazards be eliminated, reduced to the extent feasible, or materially reduced using an incremental abatement process.
4.9.1.3 Workers shall be encouraged to participate in ergonomics programs and report MSD's signs or symptoms.
4.9.1.4 Industry standards applicable to ergonomic equipment shall be considered requirements of this section.
4.9.2 Responsibilities
4.9.2.1 The OCHMO shall provide guidance and advice to NASA Centers on ergonomics.
4.9.2.2 The Director of Health and Medical Systems shall ensure Center ergonomics policy and programs are assessed for efficacy through regular, periodic reviews.
4.9.2.3 Centers shall implement an ergonomics program to ensure proper fit between the job tasks, equipment, and the worker performing the duties.
4.9.2.4 Centers shall develop and maintain effective ergonomic programs, consistent with the requirements stated herein and with current professional guidance from organizations such as OSHA and NIOSH.
4.9.2.5 Centers shall assure that industrial hygiene is involved in the selection of the computer workstations and that a member of the industrial hygiene group is involved with the procurement of computer workstations.
4.9.3 Process Description
4.9.3.1 Each Center shall have a written ergonomics program that includes at least the following elements:
a. Management support and employee participation;
b. Worksite analysis;
c. Job analysis;
d. Medical management;
e. Training; and
f. Program evaluation.
4.9.3.2 At a minimum, management support of the ergonomics program shall be demonstrated by approving a Center ergonomic policy. Workers (and their designated representatives) shall have ways to report signs and symptoms of musculoskeletal disorders (MSDs); obtain responses to reports; and participate in developing, implementing, and evaluating each element of the program. Policies or practices shall encourage workers to participate in the program and report signs and symptoms of MSDs. A method for workers to report signs and symptoms of MSDs and to get prompt response and followup shall be established. Worker reports of signs and symptoms of an MSD shall be evaluated to determine whether an MSD has occurred. Information to workers shall be periodically provided that explains how to identify and report signs and symptoms of an MSD.
4.9.3.3 A worksite analysis shall be performed in all areas where potential ergonomic hazards exist and whenever operations are introduced or modified creating the potential for new ergonomic hazards. This includes, but is not limited to, examination and tracking of injury and illness records to identify patterns of traumas or strains that may indicate the development of MSDs.
4.9.3.4 Operations with significant ergonomic risk factors present shall be analyzed to fully define the ergonomic risk factors that could result in MSD hazards. The ergonomic hazards shall be eliminated, reduced to the extent feasible, or materially reduced using an incremental abatement process.
4.9.3.5 A medical intervention and/or management program shall be designed and implemented to eliminate or reduce the risk of development of MSDs through early identification and treatment. The program shall be implemented by qualified medical providers. Concerted efforts shall be made to return workers to work as soon as possible.
4.9.3.6 Workers shall be provided proper ergonomic training to make them aware of the ergonomics program, common MSD hazards, and methods for eliminating MSD hazards.
4.9.3.7 Center ergonomic programs shall be re-evaluated at least annually and changes implemented to ensure coverage of all potential ergonomics hazards. Metrics that document the efficacy of the ergonomics program shall be maintained and used to improve the program and further reduce MSD risks.
4.10.1 General
4.10.1.1 NASA Centers shall eliminate or minimize indoor air-related hazards (i.e., visible mold, pesticides, ozone from copiers, insufficient ventilation, chemicals in open containers, outdoor sources, etc.) that may contribute to IAQ problems.
4.10.1.2 NASA Centers shall minimize the impact of construction, renovation, and maintenance activities on IAQ; resolve all IAQ problems; and communicate IAQ information to affected employees.
4.10.1.3 This section outlines the requirements to minimize the negative impact that poor IAQ can have in the workplace on worker health, productivity, morale, and absenteeism, and establishes minimum standards for all NASA Center IAQ programs with regard to complaint investigation, IAQ testing, communication of IAQ information, mold remediation, recordkeeping, and general requirements.
4.10.2 Responsibilities
4.10.2.1 The OCHMO shall provide guidance and advice to NASA Centers on IAQ.
4.10.2.2 The Director of Health and Medical Systems shall ensure Center IAQ policy and programs are assessed for efficacy through regular, periodic reviews.
4.10.2.3 Centers shall have written IAQ programs intended to ensure all indoor environments are adequately controlled for recognized IAQ-related hazards.
4.10.2.4 Centers shall ensure that their IAQ programs include provisions for:
a. Investigating IAQ complaints, conducting IAQ testing, offering technical guidance and support on minimizing the impact of construction, renovation, and maintenance activities on IAQ, recommending corrective actions to resolve all IAQ problems, communicating IAQ information to employees, remediating mold, and recordkeeping;
b. Evaluating the medical condition of workers who report signs or symptoms that they suspect may be related to indoor air contaminants;
c. Evaluating building heating, ventilation, and air-conditioning (HVAC) system designs and modifications to determine if recommended standards, including the American Society of Heating, Refrigeration and Air Conditioning Engineers (ASHRAE) guidelines are met and do not adversely affect local exhaust ventilation systems used to control hazardous materials; and
d. Evaluating housekeeping services to help ensure they are minimizing dust accumulation and food wastes and maintaining floor surfaces (including carpets) in a manner sufficient to lessen the likelihood of IAQ complaints.
e. Evaluate the process for moisture control and mold remediation to help ensure it is effective. When mold is found to be present, the Center shall develop a plan for remediation. The methods used for mold remediation depend on the type of material and the extent of the area with mold growth and shall be commensurate with current governmental, industry, and consensus guidelines and recommendations.
4.10.3 Process Description
4.10.3.1 Centers shall involve the cooperation of other internal organizations in IAQ investigations, including, but not limited to, affected individuals, IH, occupational medicine, building managers, janitorial staff, maintenance, and operations staff.
4.10.3.2 An open, transparent, and effective communication process with affected workers regarding an IAQ investigation's findings and subsequent corrective actions shall be developed and followed for significant IAQ problems. This process shall include both verbal and written communication and shall be continued until the IAQ concern is effectively resolved. Communication efforts shall start at the earliest stages of an IAQ investigation.
4.10.3.3 IAQ investigations shall follow three basic steps (these are not necessarily distinct stages and some may be intermixed depending on the situation and discretion of the investigator):
a. Identification and investigation of the IAQ concern by competent personnel. This shall be done by the appropriate IH organization;
b. Collection of appropriate and representative samples and other survey documentation; and
c. Evaluation of data, recommendations and conclusions, and report generation.
4.10.3.4 Workers shall be notified about building conditions, policies, procedures, and plans that may have a significant adverse impact (e.g., planned renovation, remodeling, and maintenance or pest control activities) on indoor air quality and operational activities.
4.10.3.5 Center EH personnel shall collaborate with facilities maintenance and operational management personnel to ensure the following additional IAQ best practice requirements are incorporated into each Center's IAQ program:
a. Construction and maintenance activities in occupied buildings shall be planned and managed to minimize the release of dust, vapors, fumes, and other air contaminants to protect workers and building occupants;
b. Building and office materials such as paint, carpet, upholstery, cushions, adhesives, and furniture shall be low/no volatile organic compound emitting and shall not significantly contribute to IAQ problems;
c. Carpets shall be maintained in an effort to ensure they do not become a source of dust, mold, bacteria, and other indoor air contaminants;
d. Integrated Pest Management principles shall be followed to minimize occupant exposure to pest- and pesticide-related contaminants and shall be used to reduce vapors and dusts created during pesticide applications;
e. Parked vehicles, such as those in loading docks, shall not be allowed to remain running in close proximity to building air intakes where exhaust contaminants may be entrained into the building;
f. Designated smoking areas shall not be near air intake systems or entry/exit doors where smoke may be entrained into the building;
g. Water spills and leaks shall be immediately attended to and water leaks reported without delay;
h. Decorative plants shall be maintained properly as to not create an environment for mold or bacteria; and
i. Water reservoirs (i.e., cooling towers, condensate pans, hot water tanks, stagnant plumbing systems such as eye washes) shall be maintained to limit biological growth.
4.10.3.6 At the conclusion of the IAQ investigation, results shall be evaluated and conclusions and recommendations derived and documented. A summary of this information shall be compiled into a report and distributed and communicated to all affected parties.
4.10.3.7 Records shall be maintained as objective evidence of compliance with this section. The following records shall be maintained for all IAQ investigations:
a. A log of IAQ complaints;
b. All IAQ interview questionnaires and forms;
c. Any monitoring and IH sampling conducted during the investigation; and
d. All IAQ reports with conclusions and recommendations.
4.11.1 General
4.11.1.1 NASA Centers shall protect the health of workers and others from the risks associated with the use of hazardous biological agents.
4.11.1.2 The scope of these requirements is limited to direct work and handling of biological hazards. This includes, but is not limited to, non-medical biological laboratory workers and animal handlers.
4.11.1.3 These requirements do not apply to potential or incidental exposure to biological hazards because of a complication to one's normal industrial work (such as a plumber or custodian) or to clinical medical functions. Such aspects shall be covered under program- or project-specific plans and procedures.
4.11.1.4 For purposes of these requirements, the hazards associated with Animal Biosafety Levels (ABSL) and the Biosafety Levels (BSLs) described in the CDC Biosafety in Microbiological and Biomedical Laboratories (BMBL) are equivalent. All BSL requirements apply to ABSLs. Equivalent control measures shall be taken to protect workers from potential exposures to animal borne biological agents. The co-application of BSL's, ABSL's, and National Institutes of Health (NIH) Risk Groups (RGs) shall be determined by a protocol driven risk assessment, and the exposure controls adjusted accordingly.
4.11.1.5 Work with prions, BSL 3 or 4, and RG 3 or 4 agents is prohibited.
4.11.2 Responsibilities
4.11.2.1 The OCHMO shall provide guidance and advice to NASA Centers on biosafety.
4.11.2.2 The Director of Health and Medical Systems shall ensure Center biosafety policy and programs are assessed for efficacy through regular, periodic reviews.
4.11.2.3 Centers shall have written biosafety programs that ensure implementation of the provisions of this section.
4.11.2.4 Center Medical Directors shall:
a. Design medical support services in consultation with representatives from the institutional environmental health and safety and principal investigators;
b. Approve all uses of BSL-1 or 2 and RG-1 or 2 agents and animals on a case-by-case basis prior to their presence on Center;
c. Approve all uses of genetically-modified agents or recombinant deoxyribonucleic acid (DNA) molecules on a case-by-case basis prior to their presence on Center;
d. Ensure the medical clinic is cognizant of potential hazards encountered by personnel working with biohazards; and
e. Evaluate affected workers previous and ongoing medical conditions, current medications, allergies (i.e., medicines, animals, and other environmental proteins) and prior immunizations, and determine what medical services are needed to permit safe performance of the duties of the position.
4.11.2.5 Environmental Health organizations shall:
a. Review and approve all proposed facility designs and equipment purchases for use with biohazardous agents prior to their procurements;
b. Review and assess procedures that impart energy to a microbial suspension or that produce aerosols;
c. Review and assess the knowledge and experience of the intended user; and
d. Inspect and certify the safety of biological safety cabinets (BSC) and other containment devices before use and at least annually, thereafter or more frequently if required by local authorities or recommended by the manufacturer to conform to the requirements of this section and NSF/ANSI Standard 49 Biosafety Cabinetry: Design, Construction, Performance, and Field Certification.
4.11.2.6 Supervisors shall:
a. Provide a description of the requirements, proposed tasks, and responsibilities of each position involving hazardous biological agents to the Medical Director to guide the medical evaluation; and
b. Cooperate with EH professionals to identify the potential worksite biohazards.
4.11.3 Process Description
4.11.3.1 The applicable recommended practices, requirements, safety equipment, training, and facility safeguards described in the latest edition of the following documents and their appendices are mandatory.
a. Centers for Disease Control and Prevention (CDC) publication, Biosafety in Microbiological and Biomedical Laboratories (BMBL);
b. NIH Guidelines for Research Involving Recombinant DNA Molecules.
c. International Civil Aviation Organization requirements for transportation of etiologic agents and infectious materials;
d. Public Health Service Foreign Quarantine regulations; and
e. National Academies Publication, Guide for the Care and Use of Laboratory Animals.
4.11.3.2 Except as otherwise defined in this document, Centers shall classify BSLs and RGs; provide applicable levels of containment; use the standard practices, safety equipment, facility, and training requirements; and handle biological agents according to the most recent recommended criteria in the CDC publication, Biosafety in Microbiological and Biomedical Laboratories (BMBL) and NIH Guidelines for Research Involving Recombinant DNA Molecules.
4.11.3.3 Centers using biologically hazardous materials, agents, and/or animals shall develop a written Biosafety Plan that outlines their approach for adhering to the mandatory requirements of all applicable regulators. The plan shall include provisions for engineering controls, administrative controls, work practices, decontamination, infectious waste management, and disposal.
4.11.3.4 Centers using biologically hazardous materials, agents, and/or animals shall develop a Biosafety Operations Manual that identifies specific hazards that may be encountered and that specifies practices and procedures designed to minimize or eliminate exposures to those hazards.
4.11.3.5 A risk assessment shall be conducted on all work with biologically hazardous materials, agents, and/or animals, including mammalian tissues or cells.
4.11.3.6 Personnel working with biologically hazardous materials, agents, and/or animals shall work under the policies and guidelines established by the Center's Biosafety Plan and Operations Manual.
4.11.3.7 The following biological agents are prohibited from use at all NASA Centers:
a. Select agents and toxins covered under 42 CFR part 73, 7 CFR 331 and 9 CFR 121;
b. Prions;
c. BSL-3 and 4 agents; and
d. RG-3 and 4 agents.
4.11.3.8 Centers shall adhere to the following training requirements when using biohazardous agents:
a. Personnel using biohazardous agents shall be trained and knowledgeable about the risks to which they may be occupationally exposed, the types of exposures that place their health at risk, the nature and significance of such risks, as well as the appropriate first aid and followup for potential exposures. Workers shall read, understand, and follow the required practices and procedures and shall consult with safety or health professionals with regard to risk assessment prior to use of those materials or organisms;
b. Refresher training shall be provided at least annually, at the time of any significant change in job responsibility, and following recognized and suspected exposures;
c. Centers conducting experiments at a BSL-1 or 2 and RG-1 or 2 shall use workers who are adequately trained and experienced;
4.11.3.9 Centers shall meet the following criteria for work involving hazardous biological agents:
a. Personnel working with human cells and tissues that are capable of transmitting disease shall be enrolled in an occupational medicine BBP program;
b. Workers using biohazardous agents shall be fully informed of the available medical support services and encouraged to utilize them;
c. Workers who may be occupationally exposed to human pathogens in research settings shall receive a pre-placement medical evaluation;
d. Medical support services for biohazards shall be based upon risk assessments and tailored to meet the organization's needs.
e. Medical support services shall be provided for all personnel equally regardless of employment status.
f. Capabilities for providing medical support for workers shall be in place before work actually begins;
g. The medical provider shall be knowledgeable about the nature of potential health risks in the work environment and have access to expert consultation;
h. Medical support services for biomedical research facilities shall be evaluated at least annually, and;
i. Joint annual review of occupational injury and illness reports by healthcare providers, environmental health, and safety representatives shall be performed to assist in revision of exposure prevention strategies to minimize biological health hazards that cannot be eliminated.
4.11.3.10 Disposal of wastes contaminated with biological agents and/or potentially infectious materials shall be handled in accordance with the Center's infectious, biological, and/or hazardous waste disposal procedures and policies.
4.12.1 General
4.12.1.1 NASA Centers shall use the latest version of the United States Department of Health and Human Services (HHS), Food and Drug Administration (FDA) Food Code, and the Hazard Analysis Critical Control Point (HACCP) methodology (prevention-oriented, science-based food safety principles) as the primary means of regulating food safety at food establishments under NASA jurisdiction.
4.12.1.2 NASA Centers shall ensure food safety through the implementation of appropriate procedures, training, and active monitoring to reduce risk.
4.12.1.3 OCHMO is the overall NASA authority for food safety and coordinates food safety matters with outside agencies.
4.12.1.4 Centers shall determine the best ways to ensure retail food establishments, see Appendix A for definition, develop procedures, effectively train their associates, and verify that those procedures are being implemented.
4.12.1.5 The Food Safety requirements contained herein apply to all retail food establishments operated by NASA or NASA Contractors.
4.12.1.6 The FDA Food Code shall be the minimum standard for controlling the risk factors known to contribute to foodborne illness at NASA Facilities.
4.12.1.7 Food safety measures established in the most recent version of Food Code shall be accomplished through the implementation of HACCP principles and risk-based inspections and controls.
4.12.1.8 Where conflicts exist between the most recent FDA Food Code, this section and any additional state or local "food code" requirements, whichever is most protective shall be applied.
4.12.1.9 Where conflicts exist between this section and any additional Center requirements, whichever is most protective shall be applied.
4.12.2 Responsibilities
4.12.2.1 The OCHMO shall provide guidance and advice to NASA Centers on food safety.
4.12.2.2 The Director of Health and Medical Systems shall ensure Center food safety policy and programs are assessed for efficacy through regular, periodic reviews.
4.12.2.3 Centers shall mitigate potential food safety hazards by establishing a primary prevention approach to food safety that encompasses planning and reviews of all proposed projects, processes, and procedures to mitigate potential food safety hazards.
4.12.2.4 Centers shall notify OCHMO of food-related incidents as soon as possible and by the most expeditious means.
4.12.2.5 Centers shall:
a. Only allow operations of food service establishments that meet or exceed the minimum acceptable requirements established by this section and applicable Federal, state, and local regulations for the safe handling of food;
b. Ensure that the requirements and provisions of this section are included in food and beverage services contracts, subcontracts, and other applicable contracts/agreements;
c. Maintain current food safety policy and procedures which assign responsibility, accountability, and authority to pertinent Center organizations, departments, and personnel;
d. Ensure the food safety program has an established system to detect, collect, investigate, and respond to complaints and emergencies that involve foodborne illness, injury, and intentional and unintentional food contamination;
e. Promote a comprehensive awareness and active managerial control over risk factors most
commonly associated with foodborne illnesses;
f. Ensure that food establishments' food safety management plans implement sound food safety practices;
g. Ensure that food establishments implement food safety management plans that incorporate active managerial controls, HACCP principles, training requirements, hygiene standards, cleaning and sanitary practices, illness reporting agreements, food hazards of significance, monitoring procedures, record keeping, corrective action processes, and proper certification of food service workers;
h. Ensure that Critical Control Points (CCPs) and Critical Limits (CLs) are included in recipes or recipes are controlled via an overall policy that is based on the current FDA Food Code and HACCP methodology and principles;
i. Ensure Center Food Safety Program elements are implemented and maintained;
j. Coordinate questionable conflicts between the latest FDA Food Code and local "food code" with the local authorities;
k. Conduct a program of continuing inspection and surveillance of all food establishments;
l. Ensure the inspection program focuses on the status of risk factors, determines and documents compliance, and targets immediate- and long-term correction of out-of-control risk factors through active managerial control;
m. Ensure program management has established quality assurance measures to ensure uniformity among inspection staff in the interpretation and application of laws, regulations, policies, and procedures;
n. Ensure that Food Safety Inspection personnel have the knowledge, skills, and ability to adequately perform their required duties;
o. Perform onsite, risk-based food safety inspections of food establishments as recommended by the FDA Food Code, Annex 5, Table 1. Inspections shall include:
(1) Identification and assessment of the hazards and associated risks.
(2) Determination of and implementation of CCPs, CLs, and procedures necessary to reduce risk of foodborne illness.
(3) Determination of active managerial controls.
p. Maintain accurate and complete survey and inspection data records for the last three months or last three inspections, whichever time span is greater, and have them available for review by inspection personnel and food installation customers;
q. Correct all inspection violations in a reasonable length of time;
r. Prominently post the most recent inspection report for customers to view or a sign or placard notifying customers that inspectional information is available for review;
s. Provide consultation in the preparation of state and/or local permit applications for food service activities;
t. Ensure compliance monitoring and reporting is carried out in a timely manner;
u. Ensure compliance and enforcement activities result in followup actions for out-of-control risk factors and timely correction of violations;
v. Maintain copies of state and/or local permits, and associated records;
w. Notify local and state health departments, the CDC, and/or the Department of Homeland Security, consistent with applicable reporting requirements, of foodborne disease outbreaks;
x. Ensure that Center Senior Management is routinely apprised of the status of major food safety issues and problems;
y. Ensure that OCHMO and the Center OH Office are immediately advised of major accidents, incidents, or emergencies involving food safety.
z. Ensure that Center policy and food safety plans require prompt notification of a responsible individual in the event of an emergency resulting in conditions that could create an imminent hazard (e.g., fire, flood, extended interruption of electrical service or water service, sewage backup, a report of foodborne illness) or any other unsanitary occurrence/condition that might contaminate food and endanger employee health.;
aa. Ensure design reviews are conducted for new or redesigned food establishments, as well as for facilities that intend to make significant changes to the existing menu or theme;
bb. Ensure that food safety personnel and food inspection personnel are included in the procurement of food establishment equipment and Facility design reviews;
cc. Provide design and procedure reviews, technical assistance, and consultation with all Center stakeholder organizations on matters concerning food safety;
dd. Ensure the review of plans by qualified individuals for temporary events that involve food and provide recommendations concerning food safety provisions;
ee. Ensure that proper food handler physical examinations are provided to food services workers as per Appendix C of this NPR;
NOTE: Centers may offer Hepatitis A inoculations to food services workers who work at food establishments on NASA property or under NASA jurisdiction at the discretion of Center Management.
ff. Ensure all food handlers report to a physician when any symptoms of infections and/or communicable diseases are present;
gg. Ensure that food service workers immediately report symptoms of illness that may be transmissible through food to their supervisor;
hh. Ensure that all food handlers returning to work after an illness-related absence associated with any of the conditions below are medically cleared:
(1) A diagnosed illness of Norovirus, typhoid fever (Salmonella typhi), shigellosis (Shigella spp.), E. coli O157:H7 infection (or other EHEC/STEC (enterohemorrhagic or Shiga toxin-producing E. coli), or Hepatitis A virus (Hepatitis A) or nontyphoidal Salmonella.
(2) Symptoms of gastrointestinal illness such as diarrhea, fever, vomiting, jaundice, or sore throat with fever.
(3) A lesion, boil, or wound containing pus that is open or draining and is located on the hands, wrists, or exposed portions of arms.
(4) Illness from consuming food that was implicated in or caused an outbreak.
ii. Identify and provide support concerning certification and training requirements for food managers and food service workers;
jj. Ensure that training is provided to maintain any certification requirements food service managers may need;
kk. Ensure all food handlers receive refresher training on a routine basis to ensure food safety principles and practices are reinforced.
ll. Remove from service or sale all food items suspected to be contaminated, unwholesome, out-of-date, or otherwise deemed unfit for consumption;
mm. Ensure that organizations operating vending machines that dispense Temperature Controlled for Safety (TCS) food or beverage items provide the Center OH Office with a list of onsite vending machines and their locations; and
nn. Ensure that vermin are controlled through an Integrated Pest Management (IPM) program that integrates housekeeping, maintenance, and pest control services to prevent the creation of a health hazard to humans. The IPM program shall be site specific and tailored to food establishment operations.
4.12.3 Process Description
4.12.3.1 Food served or vended at NASA Centers and Component Facilities shall be from approved sources that are monitored and regulated under Federal, state, or local food safety inspection programs. Food shall be protected during all stages of production to assure that it is safe and unadulterated. This applies to the receiving, transporting, storing, preparing, serving, and vending of food provided. This applies equally to all appropriated funded, non-appropriated funded, organizational, contractor, and/or private association food activities held on Centers.
4.12.3.2 Food operators shall comply with HACCP methodology and principles and the latest FDA Food Code.
4.12.3.3 Food operators shall have written food safety policies and written food safety plans (specific to establishments) that ensures that HACCP principles and methodology implements a process of self-inspection and continuous improvement. The management system shall provide for effective and active managerial control and the purposeful incorporation of specific actions or procedures into the operation of food service establishments to attain control over foodborne illness risk factors. Unique conditions within each Facility shall be considered during the development of food safety and HACCP plans. Generic plans are not acceptable. Food safety plans shall identify potential hazards of significance and include preventive measures to ensure and improve food safety. CCPs shall be effectively controlled and CLs shall be properly observed and implemented.
4.12.3.4 Constraints/controls imposed upon substances/products/operations subject to the provisions of this section shall be no less than those required by applicable regulatory authorities and shall include any additional special constraints deemed necessary by OCHMO as a result of unique or operational characteristics.
4.12.3.5 Centers shall generate, retain, and dispose of food safety records according to NASA EH records requirements found in NPR 1441.1, NASA Records Retention Schedules.
4.12.3.6 Records shall be available for review by the OCHMO and Federal, state, and/or local food safety inspectors. Examples of records include applicable training records, inspection records, walk-in refrigerator/freezer daily alarm check logs, temperature logs, food receiving logs, maintenance logs, and dishwasher logs.
4.12.3.7 New and redesigned facilities shall be reviewed by the Center OH Office and meet the principles outlined in state and local codes and the FDA Food Code. All design deviations and changes that may affect the Center's Food Safety Program requirements shall be coordinated with appropriate Center personnel and stakeholders; and approved in advance by the Center's OH representative.
4.12.4 Farmers Markets
4.12.4.1 Cottage foods and produce are the only foods that can be sold by farmers market vendors on NASA property. The following foods may not be sold:
a. Fish or other aquatic species.
b. Livestock, a livestock product, or livestock by-product.
c. Planting seed.
d. Poultry, a poultry product, or poultry by-product.
e. Wildlife processed for food or by-products.
f. A time/temperature control for safety food made from a product described in this paragraph by a farmer or other producer who grew or processed the product.
4.12.4.2 Any farmers market vendors offering produce samples (e.g., cut fruits and vegetables) will be held to local/state retail food safety requirements.
4.12.4.3 These requirements do not preclude on-site food trucks or other food retail establishments from providing foods concurrently with the farmers market but such food operations will be held to NASA and local/state retail food safety requirements.
4.12.4.4 Center Food Safety Inspectors, civil service or contractors (per the contractor's contract), shall conduct appropriate inspections at farmers markets to ensure produce vendors are managing the risk factors for food safety appropriately and following all applicable state and local codes, and cottage foods vendors are abiding by the specific state cottage food laws and other applicable state/local codes.
4.12.4.5 Center Market Managers shall:
a. Ensure food safety through the implementation of appropriate agreements, communication, and active monitoring to reduce risk when operating on NASA property.
b. Prior to participating at the farmers market, obtain from cottage food vendors:
(1) A product list of cottage foods the vendor plans to offer at the farmers market.
(2) Required state/local certifications, registrations, or licenses to operate cottage food kitchens.
(3) A vendor-signed agreement to operate following food safety practices and applicable state cottage food laws and other applicable state/local codes.
c. Ensure all cottage foods sold at the farmers market are allowed by applicable state/local cottage food laws.
d. Ensure all cottage foods sold at the farmers market are labelled according to applicable state/local cottage food laws. Typically, this signage informs customers of where the food comes from and that the operation is not subject to the state's food safety regulations.
e. Prior to participating at the farmers market, obtain from farmers or their representative (produce vendors):
(1) A product list of produce the vendor plans on offering for sale.
(2) Required state/local certifications, registrations, or licenses.
(3) A vendor-signed agreement to operate following food safety practices and applicable state/local codes.
f. Inform employees participating in farmers markets through signage or messaging that the food from the markets may come from an operation not necessarily covered by the more stringent United States Department of Agriculture (USDA) or Food and Drug Administration (FDA) Food Safety regulations or other state/local codes.
g. Coordinate with the appropriate Center safety office regarding the safe set up of vendor space regarding generators, cords, etc.
h. Establish a policy for ensuring food waste and garbage is appropriately handled and removed at the end of the market designating whether the farmers market vendors or NASA is responsible for handling waste removal. Part of this policy will include pest control and how it is handled since the food or waste may attract pests such as bees, flies, etc.
4.13.1 General
4.13.1.1 Health Physics is the application of scientific principles to the protection of workers and others from the hazards of radiation. NASA Centers shall maintain and preserve the radiological health of their workforce by minimizing occupational exposures, eliminating unnecessary exposures, and reducing the potential for accidental exposures to ionizing and non-ionizing radiation.
4.13.1.2 The OSMA maintains purview concerning the launching of radioactive materials.
4.13.1.3 Exposures to ionizing radiation shall be maintained As Low As Reasonably Achievable (ALARA) and exposures to nonionizing radiation shall be maintained ALARP.
4.13.2 Responsibilities
4.13.2.1 The OCHMO shall provide guidance and advice to NASA Centers on radiation.
4.13.2.2 The Director of Health and Medical Systems shall ensure Center radiation policy and programs are assessed for efficacy through regular, periodic reviews.
4.13.2.3 The SEHO shall recommend Agency-level radiation policy and requirements to the CHMO.
4.13.2.4 Centers shall achieve the ALARA objective by the use of active managerial controls, safe operating procedures, appropriate equipment, a comprehensive maintenance and surveillance program, adequate shielding and distance, and/or by limiting worker exposure time.
4.13.2.5 Centers shall designate in writing competent and qualified approval authorities to administer radiation protection programs.
4.13.2.6 Centers shall have centralized control and accountability over sources of potentially hazardous ionizing and non-ionizing radiation.
4.13.2.7 Centers shall ensure compliance with applicable Federal, state, and local requirements through independent quality assurance checks.
4.13.2.8 Centers shall ensure that adequate personnel, facilities, equipment, training, and operational and emergency controls are maintained for all operations utilizing ionizing or nonionizing radiation.
4.13.2.9 Centers shall ensure that radiation sources are used safely and in accordance with written procedures based on sound radiation protection and engineering principles.
4.13.3 Process Description
4.13.3.1 Centers in which operations exist that expose workers or the public to ionizing and nonionizing radiation shall administer a comprehensive radiation protection program to identify and control those radiation exposures in accordance with this section.
4.13.3.2 Radiation protection programs shall be implemented by written procedures and reviewed at least once every 12 months to evaluate their content and effective implementation. At a minimum, the review shall cover procedural compliance, technical adequacy, implementation, and effectiveness of the program.
4.13.3.3 Training shall be provided according to the following criteria:
a. Training shall be commensurate with the potential hazards and provided prior to unescorted access to restricted areas and prior to receiving occupational exposure;
b. Initial and recurrent training shall provide the knowledge, skills, and abilities necessary for maintaining radiation workers' doses below applicable limits;
c. Training shall provide workers with an understanding of the risks associated with radiation and the means for recognizing and addressing workplace hazards that may lead to increased risks; and
d. Female radiation workers who may be occupationally exposed to the ionizing radiation dose threshold (i.e., 100 millirem) and their supervisors shall receive special instructions on the potential health risks of prenatal exposure to ionizing radiation.
NOTE: Paragraph 4.5.1.3 and 4.5.3.1(f) and (g) contain additional information about exposure of female radiation workers.
4.13.3.4 Only persons qualified by training shall be authorized to use potentially hazardous ionizing or non-ionizing radiation.
4.13.3.5 Medical surveillance shall be conducted in accordance with Chapter 2 of this NPR.
4.13.3.6 A comprehensive inventory of all hazardous ionizing and nonionizing radiation sources shall be completed and verified annually.
4.13.3.7 A formalized approval process based on hazards analyses shall be implemented prior to the authorization of any source of hazardous ionizing and/or non-ionizing radiation.
4.13.3.8 To the maximum extent practicable, hazards to workers shall be eliminated by engineering design.
4.13.3.9 Procedures shall be developed and/or equipment provided to mitigate hazards that cannot be eliminated by engineering design.
4.13.3.10 Work activities shall be conducted as specified by the controlling written authorization.
4.13.3.11 Sources of potentially hazardous ionizing and non-ionizing radiation, whether in use or in storage, shall be controlled and secured from unauthorized access or removal according to the following criteria:
a. Controls shall be commensurate with the hazards and provide flexibility for consideration of other hazards (e.g., industrial safety, industrial hygiene, environmental hazards);
b. Use and storage locations shall afford adequate safety and security;
c. Restricted areas shall be established and posted to warn individuals that they are entering areas controlled for radiation protection purposes. Access shall be limited to authorized personnel; and
d. Activities involving ionizing or non-ionizing radiation determined to be a threat to health or property shall be immediately terminated.
4.13.3.12 Written operating, maintenance, service, and emergency procedures and use authorizing documentation shall be provided and maintained with ionizing or non-ionizing radiation sources for easily accessible reference. These procedures and procedural controls shall be commensurate with the hazards, activity, and the education, training, and skills of the individuals who may be exposed to the hazards.
4.13.3.13 A competent person (see Appendix A) trained to evaluate and document the magnitude and extent of radiation emissions and potential radiological hazards, and to verify the efficacy of controls and procedures shall perform surveillance and monitoring of approved facilities, equipment, and operations in accordance with the following specifications:
a. Surveillance and monitoring shall be conducted at least annually based on applicable regulatory requirements and license conditions. Surveillance and monitoring shall be commensurate with the potential for changes in the radiation fields and the potential magnitude of the changes;
b. Instrumentation that is used to perform radiation surveys shall be capable of accurately measuring the types of radiation, at the dose rates and under the environmental conditions that may be encountered;
c. Instruments and equipment used for quantitative radiation measurements shall be calibrated for the radiation measured at intervals not to exceed 12 months or per the manufacturer's recommendation;
d. When components affecting the radiation safety of a system are serviced or replaced, a qualified expert shall perform a survey of the installations to ensure continuity of adequate radiation safety; and
e. Surveillance and monitoring results shall be evaluated and investigations initiated to resolve unexpected results.
4.13.3.14 Exposures to ionizing and nonionizing radiation in excess of the applicable regulatory limits shall be reported to the appropriate regulatory authorities according to the regulations and to the SEHO by the most expeditious means.
4.13.3.15 Records shall be maintained to document conformance to this section, applicable regulations and standards, and with the provisions of Center's radiation protection programs. Unless otherwise specified in this section, records shall be retained until final disposition is authorized in accordance with NPR 1441.1D, NASA Record Retention Schedules.
4.14.1 General
4.14.1.1 The receipt, use, storage or transfer of radioactive materials, or equipment containing radioactive materials shall be controlled at all NASA Centers.
4.14.1.2 All procurement, use, transfer, and disposal of radioactive materials shall be coordinated with the designated radiation protection competent approval authority (e.g., Laser Safety Officer (LSO), Radiation Safety Officer (RSO), Radiation Safety Committee (RSC), etc.).
4.14.1.3 Exposures to ionizing radiation shall be maintained ALARA. Occupational exposure to naturally occurring radon shall be maintained ALARP.
4.14.2 Responsibilities
4.14.2.1 The OCHMO shall provide guidance and advice to NASA Centers on radioactive materials.
4.14.2.2 The Director of Health and Medical Systems shall ensure Center radioactive materials policy and programs are assessed for efficacy through regular, periodic reviews.
4.14.2.3 Center Senior Management shall designate in writing, competent and qualified personnel to administer a program for control and accountability of radioactive materials.
4.14.2.4 Center RSO and/or RSC, shall oversee ionizing radiation safety; approve radioactive material usage; ensure activities involving radioactive materials are conducted in accordance with applicable requirements; and take prompt corrective measures to appropriately manage or control hazards.
4.14.3 Process Description
4.14.3.1 Centers with operations potentially exposing workers or the public to ionizing radiation from radioactive materials shall develop written procedures to identify and control those radiation exposures in accordance with this section and the appropriate paragraphs of section 4.13.
4. 14.3.2 Operations and activities shall include reasonable controls directed toward reducing exposure, preventing the spread of radiological contamination, and minimizing the generation of contaminated wastes and the release of effluents.
4.14.3.3 Personal dosimeters that require processing to determine the radiation dose and are used to comply with dose limits shall be processed and evaluated by a dosimeter processor holding current personal dosimetry accreditation from the National Voluntary Laboratory Accreditation Program (NVLAP) of NIST.
4.14.3.4 Activities involving radioactive materials shall be conducted in accordance with applicable NRC or NRC Agreement state issued licenses for radioactive materials.
4.14.3.5 All procurement, use, transfer, and disposal of radiation-generating equipment shall be coordinated with the designated radiation protection competent approval authority (e.g., LSO, RSO, RSC, etc.).
4.14.3.6 Irradiation facilities using nonmedical x-ray and sealed gamma-ray sources shall comply with ANSI/HPS N43.3.
4.14.3.7 The following criteria shall be met for operations involving radioactive materials:
a. Procurement, use, storage, transfer, and disposal of radioactive materials shall be pre-approved by the RSO or RSC;
b. Control of radioactive contamination shall be achieved by using engineering controls and worker performance to contain contamination at the source, reducing existing areas of contamination, and promptly decontaminating areas that become contaminated.
c. Contaminated surfaces shall be controlled in a manner commensurate with the physical and chemical characteristics of the contaminant, the radionuclides present, and the fixed and removable contamination levels.
d. Contamination levels caused by ongoing work shall be monitored and maintained ALARA.
e. Contamination found in unrestricted areas should be immediately decontaminated to background levels. When it is not possible to get to background levels, the contamination levels listed in the governing NRC or Agreement State issued specific materials license documents shall not be exceeded. The Surface Contamination Values listed in Appendix D to 10 CFR 835 shall apply where contamination limits are not specified under NRC or Agreement State issued specific materials license documents.
f. When equipment or facilities that are potentially contaminated are to be released for unrestricted use, the requirements in paragraph e above provide the maximum acceptable residual levels. To the extent practicable, it is appropriate to decontaminate to below these levels. Surface contamination surveys should be conducted for both removable and fixed contamination before these facilities or equipment are released from restricted to unrestricted use, to ensure that they meet these limits.
g. A standardized method for smear testing of a relatively uniform area should be used to aid in comparing contamination at different times and places. A smear taken from an area of about 100 cm2 is acceptable to indicate levels of removable contamination.
4.14.3.8 To accomplish NASA's objective of maintaining individual doses below regulatory limits and ALARA, Centers shall establish administrative control levels below the regulatory dose limits.
4.14.3.9 Smoking, eating, and drinking are prohibited in restricted areas.
4.15.1 General
4.15.1.1 Radiation protection requirements shall be instituted for electronic radiation-generating equipment (e.g., x-ray machine, particle beams) and equipment that produces radiation incidental to its operation (e.g., electron microscope) at all NASA Centers.
4.15.1.2 All procurement, use, transfer, and disposal of radiation-generating equipment shall be coordinated with the designated radiation protection competent approval authority (e.g., RSO, RSC, etc.);
NOTE: Radiation-generating equipment is defined as devices which produce ionizing radiation without the use of radioactive material.
4.15.2 Responsibilities
4.15.2.1 The OCHMO shall provide guidance and advice to NASA Centers on ionizing radiation-generating equipment.
4.15.2.2 The Director of Health and Medical Systems shall ensure Center ionizing radiation-generating equipment policy and programs are assessed for efficacy through regular, periodic reviews.
4.15.2.3 Center Senior Management shall designate, in writing, competent and qualified personnel to administer a program for control and accountability of radiation-generating equipment.
4.15.2.4 Center RSOs and/or RSC shall oversee ionizing radiation safety; approve radiation generating equipment usage; ensure activities involving radiation generating equipment are conducted in accordance with applicable OSHA, state, and Agency requirements; and take prompt corrective measures to appropriately manage or control hazards.
4.15.3 Process Description
4.15.3.1 Centers with operations potentially exposing workers or the public to ionizing radiation from radiation-generating equipment shall develop written policies and procedures to identify and control those exposures in accordance with this section.
4.15.3.2 To accomplish NASA's objective of maintaining individual doses below regulatory limits and ALARA, Centers shall establish administrative control levels below the regulatory dose limits.
4.15.3.3 Personal dosimeters that require processing to determine the radiation dose, and which are used to comply with the dose limits, shall be processed and evaluated by a dosimetry processor holding current personal dosimetry accreditation from the NVLAP of the NIST.
4.15.3.4 The following criteria shall be met for all radiation-generating equipment:
a. Procurement, use, transfer, and disposal shall be pre-approved by the RSO or RSC;
b. Design and operation of irradiation facilities using non-medical x-ray shall comply with ANSI/HPS N43.3-2008;
c. Design and operation of installations using x-ray diffraction and fluorescence analysis equipment shall comply with the requirements contained in ANSI Standard N43.2-2001;
d. Certified cabinet x-ray systems shall be surveyed at intervals not to exceed 12 months to ensure conformance with Federal performance standards;
e. Medical x-ray systems shall be surveyed at intervals not to exceed 24 months to ensure conformance with Federal performance standards;
f. Diagnostic x-ray systems shall be operated in accordance with a 21 CFR 1000.55 conforming quality assurance program; and
g. Special considerations for particle accelerator operations shall include the presence of extremely high dose rates, high energy and heavy particles, activation products, and detection and monitoring difficulties associated with pulsed or high energy radiation.
4.16.1 General
4.16.1.1 Radiation protection requirements shall be instituted for laser and non-laser optical radiation-generating equipment (i.e., ultraviolet, infrared, and high-intensity lights) at all NASA Centers.
4.16.1.2 All procurement, use, transfer, and disposal of hazardous nonionizing radiation-generating equipment shall be coordinated with the designated radiation protection competent approval authority (e.g., LSO, RSO, RSC, etc.).
4.16.2 Responsibilities
4.16.2.1 The OCHMO shall provide guidance and advice to NASA Centers on laser and non-laser optical radiation.
4.16.2.2 The Director of Health and Medical Systems shall ensure Center laser and non-laser optical radiation programs are assessed for efficacy through regular, periodic reviews.
4.16.2.3 OCHMO shall resolve conflicts between Centers and states, the U.S. Military, and other Federal agencies.
4.16.2.4 Centers implement protective requirements for use of lasers and sources of hazardous non-laser optical radiation (i.e., ultraviolet, infrared, and high-intensity lights).
4.16.2.5 Centers operating lasers in unrestricted air space should coordinate outdoor laser mission details with, and request a Letter of Determination from, the Federal Aviation Administration (FAA) at least 30 days prior to propagation of the related mission's laser beam through the U.S. navigable airspace.
4.16.2.6 Centers operating lasers in restricted air space shall coordinate with, and obtain permission from, the controlling authority (e.g., military base command).
4.16.2.7 All outdoor laser missions shall meet the applicable requirements of ANSI Z-136.6, SAE Aerospace Standard (AS) 6029A, and the NASA Laser Safety Review Board (LSRB), including its Charter (Appendix F), and associated policies and procedures.
4.16.2.8 Except for lasers used in research, only laser products that comply with Federal Laser Product Performance Standards shall be procured or manufactured; unless a specific exemption is obtained from the FDA.
4.16.2.9 Quality assurance verification of laser output shall be obtained for all commercial off-the-shelf (COTS) lasers used outdoors following modifications with the potential to alter beam output. QA verification should include applicable laser parameters (e.g., wavelength, radiant power, energy, pulse width, pulse repetition frequency, and beam divergence).
4.16.2.10 For DoD-funded outdoor laser operations, Centers shall coordinate outdoor laser mission details with, and obtain permission from, the U.S. Strategic Command prior to propagation of the related mission's laser beam above the horizon in accordance with the
28 February 2012 AIR FORCE MEMORANDUM FOR JFCC Space/J9, entitled Satellite Protection Guidance for the Laser Clearinghouse (Appendix G).
4.16.2.11 Centers shall coordinate exemptions for Federal Performance Standards with the FDA.
4.16.2.12 Center Senior Management shall designate in writing, competent and qualified personnel to administer a program for control and accountability of laser and non-laser optical radiation sources, which shall:
a. Oversee laser and non-laser optical radiation source safety;
b. Approve laser and non-laser optical radiation source usage, including use locations;
c. Ensure activities involving laser and non-laser optical radiation sources are conducted in accordance with Federal, state, and Agency requirements; and
d. Take prompt corrective measures to eliminate hazards.
4.16.3 Process Description
4.16.3.1 Centers with operations potentially exposing workers or the public to laser or hazardous non-laser optical radiation shall develop written procedures to identify and control radiation exposures in accordance with this section and applicable paragraphs of section 4.13. Requirements shall be based on accessible emission levels and ancillary non-beam hazards.
4.16.3.2 Personnel working with class 3b and 4 lasers and hazardous sources of non-laser optical radiation shall be appropriately trained in safe work practices for controlling or mitigating personal exposures. Training shall be provided to personnel working with or potentially exposed to Class 1M, Class 2, Class 2M, or Class 3R laser radiation if planned use could potentially exceed Maximum Permissible Exposure Limits (MPELs). The level of training shall be commensurate with the degree of potential laser hazards, both from the laser radiation and non-beam hazards.
4.16.3.3 Class 3b and 4 lasers and laser systems shall require a hazard assessment and approval by the LSO and/or LSC whether indoors or outdoors.
4.16.3.4 Hazards to personnel shall be eliminated, or procedures shall be developed and equipment provided to control those hazards that cannot be eliminated by engineering design prior to source approval.
4.16.3.5 Protective measures shall be employed to ensure that personnel are not exposed to laser and non-laser optical radiation in excess of the MPE limits.
4.16.3.6 Class 1 laser systems containing embedded lasers shall be controlled according to the classification of the embedded laser when engineering controls (e.g., enclosures, interlocks) are bypassed.
4.16.3.7 The LSRB shall be the final review body for all NASA-sponsored outdoor laser operations, including laser safety launch approval for use of lasers in space, ground-based and airborne laser missions.
4.16.3.8 The LSRB shall review proposed use of all outdoor lasers under NASA purview to ensure compliance with applicable regulatory requirements and adherence to exposure limits.
4.16.3.9 The LSRB shall make recommendations to the Agency on matters related to outdoor laser use and review the use of all outdoor lasers under NASA's purview.
4.16.3.10 All outdoor laser operations shall meet the following requirements:
a. Laser safety packages shall be submitted to LSRB in accordance with the LSRB Charter, and its associated policies and procedures;
b. Have LSO and/or LSC approval prior to use;
c. Caution shall be exercised to prevent visual interference in FAA designated flight zones established around airports;
d. A comprehensive outdoor laser use assessment shall be documented in accordance with the LSRB Charter, and its associated policies and procedures;
e. To ensure against inadvertent laser emissions and to mitigate potential catastrophic events, approval of airborne laser operations shall rely on a combination of interlocks and high-speed shutdown systems, as deemed necessary by engineering analyses;
f. If software is used in conjunction with lasers, it shall require a software safety analysis per NPR 8715.3, NASA General Safety Program Requirements;
g. Centers shall advise the Agency Radiation Safety Manager of all outdoor laser coordination with the FAA, U.S. Strategic Command, and/or local military commands and shall copy the SEHO and the LSRB Chairperson on such correspondence, including requests for Letters of Determination from the FAA and all other coordination of matters arising from outdoor lasers.
h. Objections, verbal or written, to the use of specific outdoor lasers by the FAA or the U.S. Military, shall be honored until the LSRB reviews the complaint and authorizes continuation of operations.
4.16.3.11 Centers shall comply with the MPE limits for laser radiation specified in ANSI Z136.1 and the occupational exposure limits for non-laser optical radiation specified in ACGIH Threshold Limit Values for Chemical Substances and Physical Agents & Biological Exposure Indices.
4.17.1 General
4.17.1.1 Radiation protection requirements shall be instituted for electromagnetic radiation-generating equipment at all NASA Centers.
4.17.1.2 All procurement, use, transfer, and disposal of hazardous electromagnetic radiation-generating equipment shall be coordinated with the designated radiation protection competent approval authority (e.g., LSO, RSO, RSC, etc.).
4.17.1.3 NASA Centers shall implement radiation protection requirements to prevent or control potential risks associated with exposure to electromagnetic fields from RF and microwave sources that operate in the frequency range of 3 kHz and 300 GHz, including, but not limited to, radar systems; spacecraft and vehicle telemetry and communications systems; Earth stations; microwave diathermy units; radio frequency generators; and Radio Frequency (RF) heat sealers.
NOTE: Hazards of electromagnetic radiation to ordinance are beyond the scope of this document. The OSMA maintains purview regarding electromagnetic radiation and its relationship to ordnance.
4.17.2 Responsibilities
4.17.2.1 The OCHMO shall provide guidance and advice to NASA Centers on radio frequency electromagnetic radiation.
4.17.2.2 The Director of Health and Medical Systems shall ensure Center radio frequency electromagnetic radiation policy and programs are assessed for efficacy through regular, periodic reviews.
4.17.2.3 Center Senior Management shall designate competent and qualified personnel to administer a program for control and accountability of RF and microwave radiation devices, whom shall:
a. Oversee RF and microwave safety;
b. Approve RF and microwave radiation equipment usage;
c. Ensure activities involving RF and microwave equipment are conducted in accordance with applicable OSHA, state, and NASA requirements; and
d. Take prompt corrective measures to eliminate hazards.
4.17.3 Process Description
4.17.3.1 Each Center with operations potentially exposing workers or the public to non-ionizing radiation above the applicable lower tier exposure limits from RF and microwave generating equipment shall develop written procedures to identify, document, and control those radiation exposures in accordance with Institute of Electrical and Electronics Engineers (IEEE) Standard C95.7.
4.17.3.2 Techniques and instrumentation for the measurement and computation of potentially hazardous RF radiation both in the near field and the far field of the RF or microwave source, including contact voltage and contact and induced currents, shall be in accordance with IEEE Standard C95.3.
4.17.3.3 All personnel with exposures likely to exceed the lower tier exposure limit for controlled environments shall be appropriately trained in safe work practices for controlling or mitigating personal exposures.
4.17.3.4 Exposures, of the general public and workers who do not have occupational duties requiring exposure to microwave and/or RF radiation, shall be kept below the upper tier exposure limit for uncontrolled areas as specified in IEEE C95.1.
4.17.3.5 Exposures of workers whose occupational duties require exposure to microwave and/or RF radiation above that allowed in uncontrolled areas shall be kept below the upper tier exposure limit allowed in controlled areas.
4.17.3.6 Training shall be provided to workers who have occupational duties that require exposure at IEEE C95.1 defined levels, which shall include the hazards of exposure; safe work practices; concepts of "time-averaged exposure;" and the methods to reduce, eliminate, or mitigate the hazards.
4.17.3.7 Workers shall be provided with specific information from surveys or computations described in 4.17.3.8 below, and guidance to prevent exposure greater than the upper tier exposure limit.
4.17.3.8 RF and microwave radiation source approvals shall be based on documented RF exposure assessments, which include direct measurements when practicable.
4.17.3.9 Operations and activities shall include reasonable controls directed toward reducing exposure. Such controls include engineering and administrative controls as well as the use of personal protective equipment, placement of appropriate RF safety signage, designation of restricted access areas, RF safety awareness training, and the use of personal RF monitors.
4.17.3.10 The beam height of RF and microwave transmitters shall be maintained at a level that does not intercept occupied facilities or structures, or personnel within the identified hazard distance.
4.17.3.11 Limits for maximum permissible exposure and induced and contact RF currents shall be derived in accordance with IEEE Standard C95.1.
4.17.3.12 Limits for lower frequency electromagnetic fields and static magnetic fields shall be in accordance with ACGIH Threshold Limit Values for Chemical Substances and Physical Agents and Biological Exposure Indices.
5.1.1 All Centers shall ensure that Federal employees and their immediate families are provided assistance with confidential, short-term psychological assessment and referral, and short-term resolution of issues related to work and family life that may affect employee health and well-being, the safety of the employee and co-workers, or job performance, attendance, and productivity. 5 U.S.C. 7901, Health Service Programs, authorizes expansion of Agency EAPs to address other employee issues such as family, financial, and marital problems. NASA EAP services shall be private, confidential, free, and strictly voluntary. An employee may also be formally referred to a Center's EAP by his/her supervisor as a result of performance or conduct deficiency. The EAP is available to all NASA Civil Service employees and immediate family members. Depending on the Center OH contract specifications, the EAP may also be available to contractors and contractor family members.
5.1.2 Provider Contractor Statements of Work shall incorporate the requirements listed in this chapter, as well as other applicable NASA contract requirements.
issues are further protected by 42 CFR Part 2, "Confidentiality of Alcohol and Drug Abuse Patient Records." Depending on the location of EAP services, additional protection may be provided by state laws, state regulations, and/or professional association guidelines.
5.2.2 Center managers and supervisors shall inform employees about the availability and confidential nature of EAP services. During orientation and training activities, human capital representatives or EAP Officers or Clinicians shall also relay information to employees about the confidentiality policies and procedures associated with the EAP.
5.2.3 At the initial visit to the EAP, Clinicians shall inform employees about the procedures and laws affecting the EAP system of records, and employees shall be provided with a written Statement of Understanding concerning the confidential nature of EAP records. The Statement of Understanding shall contain elements reflected in 42 CFR Part 2. Instances where discreet employee information discussed in counseling may be disclosed to a third party (e.g., danger to self or others, suspected child abuse, or neglect) shall also be provided in the Statement of Understanding.
5.3.1 EAP Clinicians shall not release any information without a signed consent from the employee, regardless of the issues discussed during counseling, except when required by law.
5.3.2 The NASA EAP Administrator, EAP Clinicians, and Center EAP Officers (frequently the Occupational Health COR shall serve as resources for employees and their representatives (e.g., legal or union) for details on how to legally access EAP records.
5.3.3 Employees shall have the right to access their own EAP records. The employee shall submit a formal written request to their EAP Clinician. The exception to this requirement is, when in the clinical judgment of the EAP Clinician, it may cause additional harm to the client.
5.3.4 Regular and routine access to EAP records is limited to EAP Clinicians working directly with EAP clients.
5.3.5 The NASA EAP Manager and NASA EAP Officers shall have access to "redacted" Center EAP client records for the purposes of EAP oversight, evaluation, and quality assurance. Redacted records shall not contain any employee-identifying information and shall be appropriately sanitized by the Center EAP Clinician.
5.3.6 Records disclosure with consent (except where disclosure without consent is allowed) requires that an employee's written consent be obtained before any release of EAP information can be made. This applies to all releases, including those to supervisors, treatment facilities, and family members, without regard to the type of problem the individual is experiencing. An employee's written consent is required to discuss any confidential information with Human Capital, union representatives, and other similar offices or programs. All consent forms shall meet the requirements of 42 CFR Part 2.
5.3.7 Records disclosure without the employee's written consent is only permitted in a few specific instances. Any need for EAP records disclosure without consent shall be treated with the strictest confidence and comply with applicable Federal and individual state laws. Nothing in this chapter restricts or prevents an EAP Clinician from complying with the duty to report that which is mandated by Federal or state law. Any request or subpoena for records should be forwarded to the Office of the Chief Counsel at the applicable Center or to the Office of the General Counsel at Headquarters. The CHMO and the NASA EAP Manager shall be notified when a determination for disclosure of an EAP record without consent has been made.
5.3.8 Records disclosure may be made to individuals, such as law enforcement authorities and those persons being threatened, but the disclosure shall not identify the EAP client as an alcohol or drug abuser.
5.4.1 In cases where employees are referred to the EAP by supervisors because of work performance and/or conduct issues (except as provided in 5.3 above), no information shall be released to supervisors without the employee's written consent except whether or not employees made or kept appointments during official duty hours or any sick leave (for Drug-Free Workplace cases only).
5.4.2 Employees shall not be required to release information to supervisors (except as provided in 5.4.1 above). If employees choose to disclose their EAP file information, a consent form shall be signed by the employee to allow the release of information. The process is as follows:
a. If employees choose not to sign consent forms, the EAP shall not disclose any information to employee supervisors;
b. When employee consent is given to disclose information to supervisors, the EAP Clinician shall limit the discussion to attendance at the EAP, cooperation with the program, treatment plans that may interfere with the workplace, and work performance or conduct issues. The information provided by EAP Clinicians shall give supervisors a general idea of the kind of progress employees are making; and
c. Supervisors shall be encouraged to notify the Center EAP Clinician of any changes in an employee's work performance or conduct and any corrective actions taken, since these actions may have an impact on an employee's treatment.
5.4.3 Disclosed information shall include a written statement prohibiting further secondary/additional disclosure unless the employee has expressly provided written consent and allows for further disclosures.
5.4.4 Secondary/additional disclosure statements shall be attached to all information released in writing or sent separately if the information was released orally.
5.4.5 A copy of the signed release and a description of the material released shall be placed in the employee's EAP record.
5.5.1 The OCHMO provides NASA Centers with guidance, policy and recommendations on the implementation of EAPs.
5.5.2 The Director of Health and Medical Systems ensures regular periodic onsite reviews are conducted at Centers to assess employee assistance programs.
5.5.3 NASA Center Directors shall meet with EAP providers at least twice per year to discuss the mental health of the Center's workforce, including trends, recommendations for improving the program, and the status of Center outreach initiatives. EAP providers possess the unique expertise and insight into the Center workforce that may not be communicated adequately through another individual to the Center Director.
5.5.4 The NASA EAP Manager is an Agency position and coordinates with, provides assistance to, and communicates with Center EAP Officers. This position reports to the CHMO through the Director of NASA Health and Medical Systems.
5.5.5 EAP providers are mental health clinicians who counsel and communicate with employees to assist them with issues that may impact their performance and productivity at work. EAP providers must be licensed or certified in their state in order to provide these services. All individuals, including affiliates, who provide EAP services, shall have training in and understanding of EAP practice, alcohol and other drug problems, mental health issues, human resource and labor relations issues, and organizational dynamics. EAP Clinicians implement NASA's EAP policies and programs, including programs for counseling and assisting employees with alcohol and drug abuse problems. EAP Clinicians educate and provide guidance to Center supervisors and managers to assist them in dealing with employee work-related issues. EAP Clinicians may be Civil Service personnel or contractors.
5.5.6 NASA Center EAP Officers conduct administrative responsibilities. In some cases, due to certain Center staffing scenarios, the EAP Officer is the Center's COR or the EAP Clinician.
5.6.1 NASA Center Management shall, at a minimum, be responsible for:
a. Providing resources and EAP clinician staff sufficient to ensure an effective EAP for the number of individuals able to access the service;
b. Encouraging employees to use the EAP by making services convenient and available to employees;
c. Implementing procedures that ensure professional mental health assistance is available to Center employees during regular business hours, whenever the EAP Clinician is unavailable due to vacation, illness, offsite training, emergency, or other event wherein there is no office phone or in-person coverage. Provisions for this alternative coverage shall be outlined in the contract between NASA and the Contractor in each Center's Statement of Work.
d. Ensuring that a Critical Incident Stress Management (CISM) Program is in place;
e. Ensuring that employees dealing with critical incidents have access to EAP support;
f. Ensuring that each onsite and offsite Center EAP provider has access to a "panic" button to use in any situation (e.g., client becomes violent and provider fears for his/her safety) wherein he/she is unable to summon assistance from Security or medical using standard methods; and
g. Encouraging the Center/Facility EAP Clinician's physical attendance at one NASA-led event per year to collaborate face to face with other Center clinicians, discuss best practices, share professional expertise, and otherwise foster beneficial working relationships across the Agency.
5.6.2 EAP Officers, including those who are also EAP Clinicians shall, at a minimum, be responsible for:
a. Administrative support, including coordinating with management regarding EAP outreach and initiatives;
b. Attending Agency meetings regarding Center-wide EAP issues if funding permits;
c. Serving as a liaison between the Center and the NASA EAP Manager regarding utilization reports and data;
d. Coordinating with appropriate Center program representatives and management to establish a Critical Incident Stress Debriefing (CISD) process that includes the designation of responsibilities for all team members, including management officials, emergency operations responders, medical first responders, human capital personnel, and supervisors; and
e. Providing pre-incident planning, including CISD team member training, establishing links with community partners, and identifying at-risk populations within the Center.
5.6.3 The Agency EAP Manager shall, at a minimum, be responsible for:
a. Implementing Agency EAP plans;
b. Providing assistance to EAP professionals regarding Center-wide external training programs;
c. Providing Centers with recommendations regarding the implementation of specific Center initiatives such as smoking cessation, workplace violence prevention, and stress reduction;
d. Conducting periodic meetings with all Center EAP staff to discuss current issues, trends, staff changes, and administrative matters related to Agency EAPs;
e. Providing the status of any issues related to the Agency's EAP and the results of Center by Center utilization reports to the Agency Health and Medical Services Director;
f. Supporting CISM coordination to ensure each Center's participation;
g. Advocating for individual Center contract adjustments;
h. Assisting with Center EAP training initiatives; and
i. Periodically assessing Center programs and policies that deal with minimizing the impact of harmful stress on the workforce.
5.6.4 EAP Clinician responsibilities shall include, at a minimum, the following:
a. Serving as their Center's initial Point of Contact (POC) for EAP assistance;
b. Participating in meetings regularly scheduled by the EAP Oversight Manager;
c. Being familiar with all EAP-related laws and regulations, including NPR 3792.1B, Plan for a Drug-Free Workplace, and drug treatment/rehabilitative insurance coverage that are available to employees through the Federal Employee Health Benefits Program;
d. Being qualified and trained in counseling employees in the occupational setting and being familiar with identifying evidence of illegal drug use;
e. Being responsible for providing assessments, short-term counseling, referral, and educational and outreach activities to employees, including supervisors and managers;
f. For EAP Clinicians located offsite, being readily accessible to NASA employees and being responsible for regularly communicating and coordinating with an onsite Center representative, such as the COR or EAP Officer, to ensure the continuity and quality of the EAP;
g. Participating, coordinating, and/or contributing subject matter expertise to other Agency programs, such as Critical Incident Response, Prevention/Threat Assessment, Americans with Disabilities Act, and the Drug-Free Workplace Program;
h. Ensuring that Center management and employees are notified about available EAP programs and training offered on early intervention and awareness;
i. Offering training and consultation to employees and supervisors;
j. Establishing confidential or anonymous method to obtain Center-wide employee feedback and implement quality control measures to document the degree of effectiveness of the Center's EAP;
k. Monitoring cases to ensure that continuity of care is provided or identifying reasons the client did not complete care;
l. Collecting metrics consistent with confidentiality standards that include numbers and types of cases, referrals, and general demographic data;
m. Soliciting confidential client feedback and initiating quality control measures to document the degree of effectiveness of programs;
n. Providing utilization reports as requested to the NASA EAP Manager, either directly or through their Center's COR or EAP Officer; and
5.7.1 There are several types of EAP referrals, all of which are ultimately voluntary:
a. Self-Referral: self-seeking EAP assistance by an employee who thinks that he/she may have an issue that should be discussed with a mental health professional;
b. Management Referral: referral to the EAP by a supervisor, usually as a result of a performance or conduct deficiency, or an employee who is identified as using/abusing drugs in accordance with Executive Order 12564;
c. Self-Identification: self-seeking EAP assistance by an employee who admits to drug abuse to his/her supervisor or to others and seeks rehabilitative assistance in accordance with Executive Order 12564 prior to being identified through other means;
d. Other Referral: employee referral to the EAP by a union official, medical review officer, health professional, or through any means other than a self-referral or supervisory referral.
5.7.2 NASA employees are afforded an opportunity to meet with an EAP clinician (not all EAP offices are onsite) during normal business hours. OCHMO maintains a contract with an after-hours EAP counseling service. Between 5:00 p.m. and 8:00 a.m. on weekdays, weekends, and Federal holidays, employees may contact the after-hours vendor using a toll-free number. A professional counselor will provide short-term assistance until the Center's EAP Clinician is available.
5.7.3 EAP services shall include four types of core services:
a. Individual services shall include assessment, treatment planning, referral, short-term counseling, followup, and coordination with other NASA offices such as Human Capital regarding case planning and outcomes;
b. Managerial/supervisory services shall include assistance in employee EAP referral, employee support guidance, counseling on supporting employees returning to work, employee conduct and performance guidance, and supervisor training and education;
c. Organizational assistance shall include violence prevention, crisis management, critical incident assistance, support groups, employee orientations, education and outreach, and special auxiliary services (e.g., drug-free workplace, smoking cessation, job transitions); and
d. Administrative.
5.7.4 EAP clinicians shall work cooperatively and establish partnerships with other offices such as Human Capital, Employee Relations, Equal Opportunity, Safety, Security, and Occupational Medicine clinics in work-related issues that potentially affect employee performance.
5.7.5 Critical Incident Stress Management (CISM) Program
5.7.5.1 A CISM Program shall be developed and implemented at each NASA Center as part of other employee EAP assessments and short-term counseling services offered within an environment of confidentiality. A CISM Program addresses the immediate and subsequent impact of catastrophic events on individuals or groups. The goal of a CISM Program intervention is to minimize the occurrence of post-trauma resulting from any critical incident and to augment recovery activities for populations having normal reactions to abnormal events.
5.7.5.2 A Center's CISM Program shall be written and reviewed and updated annually.
5.7.5.3 A Center's CISM Program shall be made a part of the Center Emergency Response Plan. Examples of critical incidents that could impede an employee's ability to function include natural disasters (e.g., tornadoes, hurricanes, floods, fires and earthquakes), manmade disasters, major mission failure, terrorism, homicide, sudden death, suicide, victim or witness to violence, kidnapping, or hostage situations.
5.7.5.4 A Center's CISM Program shall include:
a. Procedures that include the following:
(1) Establishing formal methods and activities used by Center management, EAP Clinicians, Emergency Preparedness and Response personnel, Security, medical first responders, onsite medical personnel, Human Capital, and supervisors to ensure stakeholders maintain an awareness and knowledge of the Center's critical incident response management procedures and processes.
(2) Establishing, training, and maintaining a CISD team and designating a CISD Team Lead.
(3) Providing direction and coordination to the CISD team.
(4) Planning and conducting pre-crisis education and pre-deployment briefing sessions.
(5) Identifying and coordinating with local community health providers (e.g., Safety, Security, mental health professionals) to establish a resource network for CISD team members.
(6) Providing information to affected personnel regarding Center efforts to identify the scope of an incident and actions being taken to support the workforce.
(7) Establishing notification methods and timelines used for community partners during or after an incident had occurred.
(8) Handling assessment, triage, treatment, referral, and followup of affected employees for up to one year, or longer if deemed necessary.
(9) Conducting meetings and post-incident intervention planning.
b. A description of the duties of the EAP Clinician (in certain Center staffing scenarios, an EAP Clinician may also serve as the Center's EAP Officer) that shall include the following:
(1) Developing CISM procedures;
(2) Establishing, providing training for, and maintaining a CISD team;
(3) Coordinating with Center Officials to establish the process for creating CISD teams.
Team members shall generally be drawn from the Center's personnel, health, safety, and security communities;
(4) Establishing links with community partners;
(5) Outlining the responsibilities for all participants, including Management, Emergency Operations Responders, Medical First Responders, Human Capital personnel, and Center Supervisors;
(6) Identifying at-risk populations within the Center;
(7) Meeting with Center Emergency Preparedness personnel, Medical First Responders, and Management to assess impact and identify affected employees on notification of a critical incident;
(8) Compiling a list of the individuals to participate in CISD Team Member briefings;
(9) Notifying the CISD team and any community partners to establish a meeting place for the Team and participants;
(10) Leading the CISD team in providing defusing and debriefing sessions, as well as providing one-on-one interventions, referral, and followup services;
(11) Making requests to the Agency EAP Manager for additional CISD training or additional temporary EAP Clinician support to respond to a critical event; and
(12) Notifying the Agency EAP Manager of all incidents that required implementation of the CISM procedures/protocol.
c. A description of Center Management duties that shall include the following:
(1) Ensuring the Center workforce dealing with critical incidents has access to EAP support; and
(2) Ensuring that the Center maintains a written and current CISM policy.
d. A description of CISD team member duties that shall include the following:
(1) Providing CISD services under the direction of the Center EAP Officer or EAP Clinician;
(2) Assisting in identifying individuals in need of additional EAP services;
(3) Being familiar with CISM components, including procedures and protocol;
(4) Participating in initial and periodic planning meetings;
(5) Providing support for a CISD exercise following a critical incident, including followup monitoring of impacted employees;
(6) Coordinating with and executing guidance from the EAP Clinician or appointed CISD Team Lead; and
(7) Participating in debriefings for CISD team members.
e. A description of Center Emergency Preparedness and Medical First Responder Personnel responsibilities that shall include the following:
(1) Familiarization with Center CISD services;
(2) Notifying the Center EAP Officer or Clinician of critical incidents and coordinating the arrangement of meeting facilities for CISD exercises;
(3) Assisting the EAP Officer or Clinician in coordinating CISM efforts, along with a designated Human Capital Officer;
(4) Identifying impacted employees; and
(5) Participating in post-incident demobilization, defusing, and debriefing exercises, as requested by the CISD Team lead.
f. A description of Center Human Resource Officer responsibilities that shall include the following:
(1) Notifying the Center EAP Officer or EAP Clinician of any known critical incidents;
(2) Assisting in identifying individuals or groups impacted by a critical incident; and
(3) Informing supervisors and employees of the availability of CISM services.
g. A description of Center Supervisor responsibilities that shall include the following:
(1) Notifying the Center EAP Officer or EAP Clinician, along with other designated contacts (e.g., Safety, Security, medical, personnel) of any critical incidents;
(2) Assisting in the identification of individuals or groups impacted by a critical incident and providing incident information facilitating the debriefing process;
(3) Encouraging and granting time for employees to participate in Center-sanctioned CISM service; and
(4) Notifying the Center EAP Officer or EAP Clinician of any difficulties an employee may be experiencing (e.g., changes in performance or behavior) following a critical incident.
5.7.6 Workplace Violence
5.7.6.1 Pursuant to NASA's Office of Human Capital NPD 1600.3, Policy on Prevention of and Response to Workplace Violence, NASA Centers shall implement and maintain a Workplace Violence Prevention Program which provides Center Directors with the discretion of designating a Center EAP as a permanent member of the Center's Threat Assessment Team (TAT). To assist in this capacity, EAP Clinicians shall:
a. Consult the most recent version of the NASA Desk Guide for the Prevention of and Response to Workplace Violence for additional information on the Agency's workplace violence prevention procedures and resources;
b. Assist other Center offices, such as Human Capital, Security, Safety, and Public Affairs in required annual workplace violence prevention training and other awareness and prevention activities for employees;
c. Assist with the review and assessment of incidents involving psychiatric, alcohol, or drug-related behavior, or any other situation that resulted in workplace violence;
d. Ensure that stress, grief, and security concerns are addressed with employees during and after workplace violence events;
e. Consult and coordinate with the Center TAT when a potential for violence exists or an actual incident is reported;
f. Consult and coordinate with Center Incident Response teams when a potential for violence exists or an actual incident is reported;
g. Participate in CISD teams in the event of a violent situation;
h. Consult with Center supervisors to identify specific problem areas, develop action plans to resolve problems in the early stages, and encourage employees and supervisors to contact the EAP for individual counseling; and
i. Help in the prevention of workplace violence through: early involvement in organizational changes; training employees in dealing with angry co-workers and customers, conflict resolution, and communication skills; training supervisors to deal with problems as soon as they surface without diagnosing the employee's problem; making recommendations to address workplace stress and violence issues; identifying ways to deal with uncomfortable or threatening situations; discussing with employees problems that can adversely affect job performance and conduct, and help employees with other problems (e.g., marital or financial issues) that may underlie potentially violent situations.
5.7.7 Domestic Violence Awareness
5.7.7.1 NASA Centers shall conduct domestic violence awareness training programs for their workforce. Domestic violence and emotional abuse are behaviors used by one person in a relationship to control the other. Individuals may be married, not married, living together, separated, or dating. Violence may be criminal and includes physical assault (hitting, pushing, shoving), sexual abuse (unwanted or forced sexual activity), and stalking. Emotional, psychological, and financial abuses may be criminal behaviors. These behaviors can lead to criminal violence. Occurrence and severity of domestic violence may increase with stress, financial difficulties, and job insecurity.
NOTE: NASA's domestic violence policy found in NPD 1600.3.
5.7.7.2 Domestic Violence Awareness Training shall be jointly offered to the workforce by the Center/Facility EAP Clinician and Human Capital and include:
a. A review of NASA's domestic violence policy and procedures, as well as any related Center/Facility-specific policy;
5.7.7.3 All Center/Facility Occupational Medicine clinic staff and healthcare workers shall be knowledgeable about the serious nature of and physical and behavioral signs of domestic violence, requesting guidance/training from the Center/Facility EAP Clinician, whenever necessary.
5.7.7.4 The Center EAP Clinician shall provide training to supervisors about the nature and dynamics of domestic violence and how to identify possible cases by the behavior employees may be exhibiting such as unusual performance or emotional instability, or by physical evidence of trauma.
5.7.7.5 All reports of abuse shall be taken seriously and the victim referred for assistance.
5.7.7.6 Center EAP Clinicians shall provide confidential consultation to management regarding employee problems related to domestic violence.
5.7.7.7 Victim assistance provided by the Center to ensure their safety shall include:
a. Center Human Capital, Legal, and Security personnel assistance when an abuser has access to the Center at which the victim is employed;
b. Availability of information at various Center offices regarding the procedures and resources to be used (e.g., telephone numbers) for assistance. A list of community resources shall be prominently available onsite, as well as in confidentially accessible locations such as bathroom and locker facilities; and
c. Center EAP assistance to confidentially assess the risk to victims, provide contacts and telephone numbers to victims to assist them, encourage victims to memorize emergency numbers, arrange for onsite contacts if community resources are not easily available, and work with victims to develop a "safety plan" that includes:
(1) Advance preparation to leave the abusive situation such as financial planning, rehearsing the actions the victim will take when the time comes to leave, making arrangements for any children involved in the victim's home, determining any legal or enforcement assistance notification and requirements that may be needed, knowing what important documents need to be taken when leaving, and a contingency plan if the initial plan cannot be implemented.
(2) Protection during violent incidents; and
(3) Safety in the home, work, and public places.
5.7.7.8 Short-term counseling shall be available to victims of domestic violence and may involve from one to several sessions, over a discrete period of time, as determined by the EAP Clinician. Counseling does not include a clinical evaluation or diagnosis. Counseling of all employees referred to the EAP (by self-referral or supervisory referral) shall at a minimum include the following:
a. Informing clients of confidentiality rights and of the duration and type of services provided by the EAP;
b. Providing problem assessment, using constructive confrontation and short-term intervention, and assisting with providing information for referrals directed to community-based resources; and
c. Referring clients for other assistance and treatment and advising on the potential cost of outside treatment, which must be paid by the client.
5.7.7.9 Employees shall be screened for evidence or history of domestic abuse, with appropriate actions taken if domestic violence is suspected.
5.7.7.10 Where not otherwise provided in the NASA Domestic Violence policy, Centers/Facilities shall develop and implement procedures to ensure the safety of domestic abuse victims, which includes the following:
a. Maintenance of victim confidentiality;
b. Security of the victim and co-workers, especially if the abuser works at or has access to the Center/Facility;
c. Provisions for victim access to Center/Facility resources during work hours; and
d. A description of the functions of the Center/Facility EAP clinician and supervisory, medical, and Human Capital personnel in cases of domestic violence against a Center/Facility employee.
5.7.8 EAP Quality Assurance
5.7.8.1 Onsite reviews of NASA Center EAPs shall be conducted in accordance with the requirements contain in Chapter 7 of this NPR. Reviews shall include, but not be limited to, an assessment of:
a. EAP staffing levels;
b. Annual internal (e.g., self-evaluation) or third party EAP evaluations during off-years in which an onsite OH review is not conducted;
c. Whether the EAP is meeting Agency objectives and goals;
d. EAP utilization rates and trends;
e. EAP availability and accessibility and conformity with NASA's culture;
f. Workforce satisfaction with program services;
g. Overall program effectiveness;
h. Maintenance of a Center-specific EAP Web site (where applicable);
i. Types and frequency of outreach and education programs;
j. Frequency of EAP and Center Management meetings to discuss status of workforce mental health;
k. Status of partnerships with other Center offices such as Human Capital, Equal Employment Opportunity, Security, Medical, Fitness, Work/Life, and Workers' Compensation;
l. Case records maintenance and quality assurance;
m. Maintenance of EAP policy and procedure documents; and
n. Timeliness and content of the EAP Utilization Report submittal.
5.7.9 Records Confidentiality, Maintenance, Retention, Coding, Security, and Destruction
5.7.9.1 NASA EAP records are considered personal case files consisting of electronic records, handwritten notes, letters to physicians or counselors, calendar of treatment(s), authorization releases, after care information, and telephone messages. EAP records, whether written, verbal, or electronic, are covered by this NPR. This NPR covers records generated and/or maintained by NASA, civil servant, or contractor EAP Clinicians.
5.7.9.2 All EAP records (electronic and hardcopy) are the property of NASA, including records created and maintained by contractors. Contractors are only the custodians of EAP records while under contract to NASA. At contract termination, contractors shall return original records to the successor EAP Clinician or the NASA EAP Administrator, consistent with the confidentiality requirements and as specified in individual Center contracts.
5.7.9.3 NASA EAP records shall be maintained in a discrete secure location and not with employee medical records, personnel files, or any other system of records in NASA. EAP case files (paper and electronic) are to be maintained in accordance with the confidentiality requirements of 42 CFR Part 2 and the requirements of the Privacy Act, in addition to other more stringent protections that may be required by local, state, or NASA Center/Facility-specific policy. All hard-copy written case records are kept in separate, secure filing cabinets that are locked when not in use.
5.7.9.4 Where an external EAP provider maintains EAP records for a NASA Center, the records shall be maintained separate from other customers' client records and be accessible for NASA OCHMO quality assurance reviews and onsite OH reviews.
5.7.9.5 EAP Clinicians shall maintain a record of cases and activities on a calendar year basis (January 1-December 31).
5.7.9.6 Records shall be retained until five years after employees have ceased contact with the EAP, regardless of whether or not employees have terminated employment with NASA. At a minimum, management referral cases shall be destroyed five years after the last date in file, or upon termination of employment. At a minimum, voluntary referral cases shall be destroyed two years after the last date in the file, or upon termination of employment. Records shall be retained longer if required by state laws where the records are stored, or until any litigation involving the employee is resolved. EAP records retention is governed by NPR 1441.1, NASA Records Retention Schedules.
5.7.9.7 To ensure confidentiality, all records shall be maintained and retrieved by unique case numbering systems rather than by names. Case-coded files shall include records that have been closed but not yet destroyed.
5.7.9.8 Each employee participating in the EAP shall be assigned a unique case number.
5.7.9.9 All hard copy case materials shall be placed in a folder and labeled with this unique case number. Computer files shall also be labeled with this unique case number.
5.7.9.10 The list of unique case numbers that correspond to the employees' names shall be maintained in a locked or secure file, separate from the case folders. It shall be secured when not in use and shall be maintained by EAP Clinicians or authorized EAP record custodians.
5.7.9.11 Identifying information recorded in case records shall be kept to a minimum.
5.7.9.12 All contacts shall be recorded with the most recent information filed on top. Entries shall only contain the information necessary for handling cases.
5.7.9.13 All persons having access to the files shall have previous training in the proper handling of records covered by these requirements. Refresher training shall be provided in the event of a requirement change.
5.7.9.14 The EAP Clinician or approved EAP record custodian shall be responsible for ensuring that file cabinets are secure before leaving each day.
5.7.9.15 Confidentiality safeguards shall be implemented with the storage of electronic EAP records in accordance with NPR 2810.1A, Security of Information Technology requirements.
5.7.9.16 Paper records shall be destroyed at the individual NASA EAP sites and in accordance with a method that has been approved by NASA.
5.7.9.17 Names of the employees whose EAP records were destroyed shall be added to a record of former EAP clients. This list shall be kept with the unique case number record and handled according to the same confidentiality procedures. No other information about clients shall be maintained once their records have been destroyed.
5.7.10 EAP Report Requirements
5.7.10.1 EAP Clinicians shall employ NASA approved EAP system-of-records software to record case data and generate reports.
5.7.10.2 Onsite and offsite EAP Clinicians shall electronically provide an annual utilization report of the previous calendar year cases to their Center management and to the NASA EAP Manager by January 31, or as requested. Data provided in the report shall include:
a. Number of cases;
b. Breakout of cases by demographics (NASA Employees, Contractors, Dependents);
c. Age and gender of clients;
d. Presenting problems;
e. Assessed problems;
f. Average number of sessions;
g. Case disposition at closure;
h. Number of management referrals;
i. Number of high-risk cases such as those involving potential workplace or domestic violence, drug or alcohol concerns, and suicidal/homicidal ideation;
j. Number of management consultations;
k. CISD and other CISM activity;
l. Training offered;
m. Support/psycho-educational groups;
n. Work-Life cases such as Child Care, Elder Care, Financial Services, Legal Services, Concierge (where provided);
o. Online and Internet resources;
p. Quality assurance activity;
q. Narrative on Center trends affecting job performance;
r. How clients heard about the Center's EAP; and
s. Recommendations.
5.7.10.3 Onsite and offsite EAP Clinicians shall also provide specialized electronically generated reports at the request of the CHMO or the NASA EAP Manager for special projects on an as needed basis.
6.1.1 The FECA provides for the payment of workers' compensation benefits for temporary and long-term disabilities to civilian officers and employees of all branches of the Government of the United States due to employment-related injury or disease. Benefits include compensation for wage loss, schedule awards, medical and related benefits, and vocational rehabilitation. FECA also provides for payment of monetary compensation to survivors of employees whose death resulted from a work-related injury or illness. The FECA is a remedial self-insurance system, with proceedings under it categorized as non-adversarial.
6.1.2 The responsibility for administering the FECA is assigned to the Director of the Department of Labor (DOL) Office of Workers' Compensation Programs (OWCP). The Director, OWCP, and his/her designees have the exclusive authority to administer, interpret, and enforce the FECA provisions.
6.1.3 NASA as a Federal Agency is responsible for:
a. Assisting with employees' timely submittal of claims to DOL;
b. Ensuring that Agency staff who handle compensation claims are adequately trained;
c. Submitting to OWCP all relevant and probative factual and medical evidence in its
possession;
d. Ensuring that facts surrounding each injury and illness are adequately investigated to
determine the validity of claims;
e. Obtaining medical status information from OWCP or injured employees as often as
necessary, within OPM and OWCP regulations;
f. Assessing employees' potential return to regular, light, or limited duty and advising
employees' physicians of any light-duty assignments or modified positions available;
g. Monitoring chargeback billings to ensure accuracy and awareness among stakeholders;
h. Staying in contact with injured employees while they are receiving compensation; and
i. Establishing organized recordkeeping systems to maintain copies of claim forms, medical
reports, correspondence, and other compensation claim-related materials.
6.1.4 Other facets of FWC benefits and how they are handled in concert with OPM benefits (e.g., disability benefits, disability annuities, benefits election) are described in the DOL Claims Examiner Procedure Manual located on the DOL OWCP Web site.
6.1.5 FWC claim processes and requirements detailed in Appendix H shall be considered part of this Chapter.
6.2.1 The President of the United States periodically directs Federal agencies to comply with specific annual targets and deadlines related to employee injuries, illnesses, and return to work rates (e.g., SHARE, POWER).
6.2.2 Executive Order 13548, Section 3, requires that agencies make special efforts to improve, expand, and increase successful return to work outcomes for employees who sustain work-related injuries and illnesses under FECA, by increasing the availability of job accommodations and light or limited duty jobs, removing disincentives for claimants to return to work, and pursing ways to foster improved return to work outcomes.
6.2.3 NASA Centers shall comply with any mandate, order, or initiative set forth by the President or DOL related to the implementation of the FECA.
6.3.1 The FECA program is financed by the Employees' Compensation Fund and is managed by the DOL and OWCP. Costs of employee workers' compensation paid out of this fund are charged back to employing agencies annually at the end of the DOL fiscal accounting period that runs from July to June.
6.3.2 Annually, OWCP sends NASA a bill with a list of FECA-related payments (e.g., medical, compensation, schedule awards) made from the fund on behalf of NASA employees.
6.3.3 Chargeback costs paid to DOL by NASA each fiscal year cover the costs incurred two years previous. Annual chargeback cost trends are used by NASA to estimate the amount designated in its budget requests to Congress. The sums appropriated by NASA are then deposited in the fund.
6.4.1 The OCHMO provides NASA Centers with guidance and recommendations on the implementation of FWC programs.
6.4.2 The Director of Health and Medical Systems ensures regular periodic reviews of the FWC case management at the Johnson Space Center for astronaut claims and the NASA Shared Services Center (NSSC) for all other NASA site claims.
6.4.3 The Agency's FWC Manager is a civil service employee who works in the NASA CHMO, Health and Medical Systems (H&MS) Division. The FWC Manager provides information and guidance Agency wide regarding OWCP requirements and serves as the liaison to DOL for the FWC program. The Agency FWC Manager reports to the Director of H&MS.
6.4.4 NASA Center management monitors chargeback costs incurred for their location, illness and injury trends that potentially impact overall employee safety and productivity, and notifies the Agency FWC Manager of any cases that may be of concern (e.g., high visibility, sensitive) or require additional considerations.
6.4.5 NASA Injury Compensation Specialists (ICS's) may be civil service employees or contractor employees located at the NSSC. ICS's conduct FWC case management for the entire eligible NASA workforce. Contractor ICS's work closely with civil service employees knowledgeable in FWC.
6.4.6 Center Occupational Medical Clinic staff serve as the medical points of contact and provide expertise when assisting ICS's with injured employee FWC medical claim-related documents.
6.4.7 Center Safety representatives provide claim-related information and evidence to ICS's regarding investigations, circumstances, and details related to employee injuries.
6.4.8 Supervisors of injured or ill employees interface and communicate with other FWC Program stakeholders, including Safety, Medical, Human Capital, and ICS's. Supervisors are usually the first individuals to be notified about an employee's occupational-related injury or illness. Supervisors inform employees of their right to file for Federal Workers' Compensation benefits.
6.4.9 Center Human Capital representatives serve as points of contact for injured employee supervisors and ICS's to identify return to work opportunities, provide employee job descriptions, and provide information about options for offering permanently disabled employees alternative or modified work environments. Center HR Specialists develop and extend job offers to disabled employees.
6.4.10 NASA payroll offices identify and transmit continuation of pay information to ICS's and coordinate with ICS's to determine NASA costs and hours for lost work days.
6.5.1 Agency FWC Manager responsibilities shall include:
a. Serving as NASA's primary liaison with the DOL and OWCP;
b. Determining and assigning ICS level of access to DOL databases and systems (e.g., Employees Compensation Operations Management Portal (ECOMP), Agency Query System (AQS), Agency Reviewer Imaging [Ari]);
c. Providing analytical data related to occupational-related injuries and illnesses to the H&MS
Director and other NASA Center FWC stakeholders;
d. Communicating changes in OWCP requirements/procedures/guidelines to appropriate
entities and individuals Agency wide;
e. Training ICS's on specific information and processes used for FWC case management and
electronic systems;
f. Notifying OWCP of errors in chargeback billing;
g. Establishing internal requirements for the Agency FWC Program;
h. Transmitting additional information to ICS's regarding illness and injury reports received
from Safety;
i. Participating in periodic training and/or attending FWC-specific meetings to remain current
on DOL policies, regulations, and initiatives;
j. Ensuring a process is in place to assist employees in the event of a (1) NASA shutdown, (2)
furlough, or (3) weather related event that may cause an interruption of service at the NSSC; and
k. Coordinating with the various Center Office of Inspector General representatives whenever a
NASA FWC case is recommended by an ICS for investigation.
6.5.2 NASA Center management shall ensure that representatives from the Centers' Occupational Medical Clinics, Safety, and Human Capital collaborate and communicate with ICS's to facilitate successful case management and employees' return to work in limited, light, or full capacity based on employees' medical status.
6.5.3 Center Occupational Medical Clinic staff responsibilities shall include providing ICS's with employees' claim-related medical information required to file claims, including information related to employees' pre-existing conditions. Medical clinic staff shall also provide assistance to ICS's to decipher claim-related medical diagnoses and physician notes and provide feedback and assistance in determining injured employees' potential return to work options.
6.5.4 Center Human Capital Office responsibilities shall include working with ICS's and providing documentation (e.g., position descriptions, potential accommodations) that will expedite returning employees to work in some capacity, based on their medical status.
6.5.5 NASA payroll offices shall assist ICS's in identifying continuation of pay (COP) hours and costs incurred for reporting to the Agency FWC Manager.
6.5.6 Center Safety representatives shall provide information and investigatory details to ICS's and injured employee supervisors to be submitted with FWC claims.
6.5.7 Supervisors of injured employees shall review and complete required FWC forms and assist ICS's and Human Capital representatives to identify light-duty and modified jobs for employees who are eligible for return to work in some capacity based on their medical status. Other responsibilities of supervisors shall include:
a. Ensuring employees are informed of their right to file a claim;
b. Directing employees to the NASA Center onsite medical clinic, when necessary; and
c. Relaying claim-related information to ICS's that may be included with paperwork
transmitted to the DOL, such as: diagrams showing where injuries occurred, verification of the time of injuries, the employee's purpose for being on premises at the time of injury, a description of the presence of witnesses, verification whether the employee was on official duty at the time of injury, and statements disputing the claim or supporting controversion of COP.
6.5.8 ICS responsibilities shall include:
a. Assisting employees with claim paperwork in accordance with OWCP mandated timelines,
procedures, and methods, including forms CA-16, CA-1, CA-2, and CA-7;
b. Assisting injured-employee supervisors with completion of claim forms;
c. Taking initial and periodic refresher training administered by an OWCP district office or
equivalent;
d. Proficiently using DOL electronic Web-based systems (e.g., AQS, ARi, ECOMP) to
complete, submit, and review NASA employee claims status, in accordance with confidentiality, security, and privacy rules;
e. Coordinating and communicating regularly with the Agency FWC Manager;
f. Tracking and reconciling continuation of pay hours, costs, and compensation and medical
costs for all active Center cases;
g. Maintaining paper and electronic records of employee claims pursuant to DOL requirements
and methods;
h. Providing FWC active case reports to each NASA Center Director and other Center
management in a format determined by the Center, whenever requested;
i. Maintaining the current status of, and documenting the progress for, claimant injury/illness
and return to work capabilities;
j. Informing Center supervisors and employees about their responsibilities and rights
concerning on-the-job injuries and illnesses which may be accomplished through new employee orientations, descriptions in employee handbooks, Web-based training classes, and similar methods;
k. Supporting and maintaining communication with employees, employee supervisors, and
NASA medical clinic representatives throughout the FWC treatment and return-to-work process, including monitoring appropriateness and effectiveness of medical care being provided, assessing employee compliance with treatment recommendations, and facilitating employees' return to work within medical limitations;
l. Reviewing quarterly DOL chargeback reports to identify errors and issues that require further research and reporting them to the Agency FWC Manager as soon as possible;
m. Reviewing second opinion medical reports and/or requesting assistance from the Center medical clinic to review claimant medical reports or interpret medical evidence;
n. Reviewing case documents for discrepancies or flagging information that seems inappropriate and notifying the Agency FWC Manager about the concerns;
o. Requesting the OWCP Claims Examiner consider mandating a second opinion medical exam or referee medical exam;
p. Reviewing cases quarterly on the periodic rolls to determine whether the claimants' or survivors' status has changed due to death, return to work (limited or full time), or a change in medical status so that NASA can research the possibility of closing cases or arrange for an offer of employment to the claimant;
q. Recommending to the Agency FWC Manager cases that warrant further review by the Inspector General's office;
r. Identifying and communicating to the Agency FWC Manager issues that appear to be impeding the ability to return an employee to work, the ability to obtain a supervisor's signature on a claim form, the ability to obtain medical authorization for an employee's treatment, and other situations that could impact assistance to the employee in obtaining treatment or the timeliness of filing a claim to the DOL;
s. Ensuring that the Agency FWC Manager is aware of ICS's communications with the DOL, aside from routine communications with claims examiners;
t. Providing guidance to injured employees' medical providers regarding the claims billing process and DOL's requirements;
u. Emphasizing and communicating to injured employees' medical providers of the availability of modified work positions and/or telework opportunities;
v. Periodically reviewing the DOL/OWCP Web site to learn of new regulations, requirements, training opportunities, and revisions to Agency reference documents;
w. Consulting DOL manuals, procedures, and guidance to research answers to case management questions;
x. Completing the Agency FWC Manager's quarterly request for new case information (COP costs/hours, injury details, age, and gender of claimants, etc.) using the template/format provided;
y. Ensuring that injured employees are informed about WebTADS and how to record COP; and
z. Reviewing cases to determine whether COP controversion is appropriate.
aa. Immediately notifying the Agency FWC Manager of any employee deaths, multiple injuries/illnesses from events likely to result in multiple claims, schedule awards for injuries/illnesses in excess of $25,000, or acceptance of any hearing loss claims;
bb. Advising OWCP if an employee's pay rate includes elements of pay such as night and Sunday differential and whether the employee has received the increments regularly (in which case the biweekly amount should be stated) or sporadically (in which case the employee's entire earnings in the relevant pay category for the year preceding the injury should be stated);
cc. Notifying, in writing, the OWCP claims examiner/district office when an injured worker returns to work and ensuring that the Agency FWC Manager is copied on the correspondence;
dd. Providing special assistance to non-appropriated fund employees with their claims since they work for private entities; and
ee. Communicating to the NASA workforce about the process and procedures in place to handle FWC-related actions and activities if there is an Agency-wide shutdown/furlough or other event (e.g., weather-related) that impacts ICS's ability to personally assist employees with claims.
6.5.8.1 NSSC ICS's' responsibilities on a case-by-case basis shall include:
a. Assisting employees who have received collection notices for DOL's non-payment of medical bills to determine whether incorrect medical provider coding is the cause;
b. Providing a list of medical providers that are known to accept FWC cases for the injured employee to review;
c. Finding out from the injured employee if he/she has contacted NASA's medical evacuation vendor to render medical assistance and/or transportation when an employee becomes ill or injured while on international travel status; and
d. Periodically researching other sources of information (e.g., obituaries, local newspaper articles) to identify potential changes in periodic roll claimants' status.
6.6.1 NASA civil service employees are covered by the FECA.
6.6.2 Coverage is extended to civil service employees regardless of the length of time on the job or the type of position held. Probationary, temporary, and term employees are covered on the same basis as permanent employees. Part-time, seasonal, and intermittent employees are also covered.
6.6.3 The OWCP has determined that employees of exchanges operated by NASA and employees who work in cafeterias and other facilities designed for the welfare of NASA employees are considered civil service employees under the FECA.
6.6.4 Special circumstances may apply to contract employees, volunteers, and loaned employees; the DOL determines compensability.
6.7.1 Civil service employees are not required to file FWC claims if they are injured or become ill at work; it is strictly their decision to file; however, employees shall report all job related injuries or illnesses to their supervisors.
6.7.2 NASA employees shall never be asked to enter into any agreement (oral or written), either before or after an illness or injury, that would waive his or her right to claim compensation under the FECA. No waiver of compensation rights shall be valid.
6.7.3 NASA shall never prevent employees from filing claims under any circumstances, nor give employees the impression, directly or indirectly, that the Agency has the authority or ability to adjudicate a claim.
6.7.4 NASA shall never suggest or recommend to an employee that he/she not file a claim, regardless of the nature of the injury or accident, circumstances, or perceived validity of the claim. NASA may provide evidence (witness statements, photographs, copies of investigative reports, medical reports) to submit to OWCP if a claim's validity is questioned.
6.7.5 Claims in process within NASA shall never be delayed due to the claimant or NASA not providing supporting documentation. Supporting documentation can be submitted to the DOL electronically or in hard-copy after the initial claim form is completed, signed, and transmitted.
6.8.1 The DOL determines whether a claim submitted is compensable, and some unique claims are adjudicated on a case-by-case basis depending on timeliness, circumstances, and evidence provided. Detailed criteria regarding compensability is located in 20 CFR Part 10 Claims for Compensation under the FECA, as amended. In general, claims meeting the following criteria would be compensable:
a. A "performance of duty" injury or illness occurs on NASA's premises during working hours
while an employee is performing assigned duties or engaging in an activity reasonably associated with their employment. On-premises coverage extends to an employee's use of facilities for comfort, health, and convenience, as well as eating meals and snacks provided on the premises. On-premises includes areas immediately outside an employee's workplace, such as steps or sidewalks if they are Federally-owned or maintained. Coverage extends to employees who are on the premises for a reasonable time (e.g., 30 minutes) before or after working hours;
b. An employee is injured while engaged in formal recreation for which he or she is paid or is
required to perform as part of training or assigned duties;
c. An employee engaged in informal recreation, such as jogging, is injured while on NASA's
premises; and
d. An employee who momentarily steps outside the sphere of employment and is injured after
assisting in an emergency, such as to extinguish a fire or help a person hit by a car.
6.8.2 In general, claims for employees performing assigned duties offsite are also compensable, such as:
a. Running official government-related errands;
b. Conducting special missions;
c. Teleworking; and
d. In-travel status. Coverage is 24 hours per day for all activities incidental to the work
assignment (but not recreational or sightseeing trips), including obtaining meals, using the hotel room, and traveling between the hotel and worksite. Claims filed should include a copy of the employee's travel orders.
6.9.1 Per 20 CFR, Section 10.11, all records relating to claims for benefits filed under the FECA, including any copies of such records maintained by NASA, are covered by the Government-wide Privacy Act system of records entitled DOL/GOVT-1. This system of records is maintained by and under the control of OWCP; all records covered by DOL/GOVT-1 are official records of OWCP.
6.9.2 The protection, release, inspection, and copying of employee claim records covered by DOL/GOVT-1 shall be accomplished in accordance with DOL rules, guidelines, and provisions, as well as those contained in 29 CFR parts 70 and 71, and with the notice of the system of records and routine uses published in the Federal Register.
6.9.3 All copies of documents in DOL/GOVT-1, including original forms and duplicate copies maintained by NASA ICS's, are governed by DOL. Documents are subject to the routine uses published in DOL/GOVT-1 and subject to the DOL's interpretation of its own routine uses.
6.9.4 NASA ICS's shall have access to FWC files by virtue of their routine use under DOL/GOVT-1, which permits disclosure, but requires handling information with care.
6.9.5 All records relating to claims for benefits are considered confidential and may not be released, inspected, copied, or otherwise disclosed except as provided in the Freedom of Information Act and the Privacy Act of 1974 or under the routine uses provided by DOL/GOVT-1, if such release is consistent with the purpose for which the record was created.
6.9.6 ICS's shall be located in separate, permanent, solid-walled (not portable/cubicle/modular) offices where injured employee personal and medical data can be reviewed and discussed on the telephone confidentially with claimants, medical providers, and the DOL.
6.9.7 Per the NASA and DOL Memorandum of Understanding Rules of Behavior, employees' confidential and/or sensitive claimant information shall be protected from disclosure. ICS's computer monitors shall not directly face an area that could allow an unauthorized person to see the contents displayed on the screen. An unauthorized person is defined as anyone who does not fall into the routine use category of individuals authorized to access FWC data.
6.9.8 FWC case information containing an employee's personally identifiable information that needs to be transmitted electronically (e-mail) shall be sent only when necessary and by using encryption (public key infrastructure) mechanisms.
6.10.1 Documents in an employee's FWC case file shall include medical reports, copies of letters and decisions, and any other material which is part of the claim, regardless of its source. These documents shall be maintained in folders apart from the employee medical folder (EMF) or Official Personnel Folder.
6.10.2 Employee case files shall not be considered a "system of records" but classified as an alternate location for the records which always remain under the jurisdiction of OWCP.
6.10.3 A notice of injury not filed with OWCP (e.g., first aid) shall be placed in the employee's EMF and retained in accordance with OPM regulations governing disposal of the EMF.
6.10.4 Any request to amend a record covered by DOL/GOVT-1 shall be directed to the OWCP District Office having custody of the official file. NASA does not have the authority to issue determinations with regard to requests for the correction of records contained in or covered by DOL/GOVT-1. Any request for correction received by NASA shall be referred to OWCP for review and decision.
6.10.5 ICS's shall maintain case file records in a secure and locked location. Records shall be stored and locked in a file cabinet or drawer whenever the ICS leaves his/her desk.
6.10.6 NASA case file copies shall be retained until three (3) calendar years after case closure, after which all copies of records shall be disposed of securely, shredded, or burned except for claim forms with original signatures (e.g., Form CA-1, Form CA-2, Form CA-5, Form CA-7, CA-7a).
6.10.7 Injured employee and injured employee supervisor original find forms shall be retained securely in a retrievable manner for 15 years after the case files have closed per DOL/GOVT-1 requirements.
6.10.8 Exceptions to destruction requirements after case closure are discretionary. Typical candidates for longer retention include cases with a clear likelihood of a schedule award that has not yet been claimed, or cases where experience shows that there may be long-term residuals requiring medical intervention in the future.
6.10.9 A claimant seeking a copy of his/her official FECA file may: (a) send a written request to the OWCP and/or (b) provide a written request to a NASA ICS. NASA shall inform claimants that any request sent to the OWCP should reference the claimant's case number on the top of every page of the request. Claimants are entitled to one free copy of their case from OWCP under the Privacy Act, with updates by written request at no charge.
6.10.9.1 Claimants requesting a copy of their file from the NASA ICS shall be informed that the file may not be complete, since the OWCP is the owner of the official case file and may have additional documents not in NASA's possession.
6.10.9.2 For any documents provided to the claimant by NASA, the NASA ICS shall implement a secure means to provide the documents to the claimant to ensure they are transmitted confidentially and with written confirmation/verification of receipt by the claimant who requested his/her case file.
6.10.9.3 Documentation and details about the issuance of case document copies to the claimant shall be retained in the claimant's NASA case file, with a copy uploaded electronically to ECOMP for inclusion in the official OWCP case file.
6.10.9.4 All requests for file copies shall comply with the rules and regulations of the DOL that govern aspects of safeguarding individuals' case records.
6.11.1 Federal Workers' Compensation Claims are typically submitted for either traumatic injuries or occupational disease/exposure/illness. Employees complete and submit form CA-1, "Federal Employee's Notice of Traumatic Injury and Claim for Continuation of Pay/Compensation" or form CA-2, "Notice of Occupational Disease and Claim for Compensation."
a. A traumatic injury is one that can be pinpointed to have occurred during one particular work shift; and
b. An occupational disease is a medical condition that has developed due to work activities performed over more than one work shift.
6.11.2 Every work-related injury or illness shall be reported to an employee's immediate supervisor. The supervisor or the onsite OH medical clinic staff shall inform the employee of his/her right to file a FWC claim and refer them to an ICS for assistance.
6.11.2.1 Pursuant to 5 U.S.C. 8101 et seq. and detailed in the Department of Federal Employees' Compensation (DFEC) Procedure Manual, employees working from home have the right to file a claim if injured while performing official duties.
6.11.3 Whenever possible, employees shall seek treatment onsite at their NASA Center clinic.
6.11.4 Any qualified physician may provide initial treatment of a work-related injury in an emergency.
6.11.5 Physicians employed by or under contract to NASA may examine the employee in accordance with OPM regulations. The employee's Center OH medical clinic staff shall obtain the employee's history, assess the injury or illness, and provide treatment if it is within the scope of the facility's capabilities.
6.11.6 The employee's choice of physician shall be honored, and treatment by the employee's physician shall not be delayed for the purpose of obtaining an Agency directed medical examination.
6.11.7 ICS counseling of injured employees about the claims process shall include:
a. An explanation regarding the confidentiality of the employee's case, especially handling of personal medical information, HIPAA, and DOL/GOVT-1 routine uses of case file data, and where applicable to HIPPA;
b. Advising the employee, orally and in writing, as soon as possible of his or her obligation to return to work under 20 CFR §10.210;
c. Advising the employee of the right to his or her initial choice of physician;
d. An explanation regarding restrictions (OWCP authorization required) associated with
claimants changing their treating physician after their initial choice. NASA cannot authorize an employee's change of physicians;
e. An explanation of what the OWCP expects to see in a medical report from the treating
physician: dates of examination and treatment, employee history, physical findings, results of diagnostics tests, diagnosis, course of treatment, other conditions found but not due to the claimed injury, treatment given or recommendation for claimed injury treatment, medically-based physician's opinion as to the causal relationship between diagnosis and factors or conditions of employment, extent of disability affecting employee's ability to work due to injury, and the prognosis for recovery;
f. Informing employees that they are required by DOL to advise NASA immediately of
their doctor's instructions concerning their return to work; and
g. Informing employees that COP or compensation may be terminated if an employee refuses work that is within his/her medical restrictions without good cause, or if he/she does not respond within specified time limits to a job offer.
6.11.8 "First aid" injuries include those requiring two or more visits to a medical facility for examination or treatment during non-duty hours beyond the date of injury, as long as no leave or COP is charged and no medical expense is incurred.
6.11.9 If an employee is examined or treated at a NASA Center's OH medical clinic or by medical providers under contract to NASA, and the examination or treatment occurred during working hours beyond the date of injury, the employee's supervisor should check "first aid" in block 39 of the Agency's portion of the CA-1 form and the CA-1 shall be submitted to OWCP via ECOMP.
6.11.10 A copy of the CA-1 form for first-aid only shall be provided to the Center's OH medical clinic for inclusion in the employee's EMF. Retaining a copy of the report in the EMF and submitting a first-aid only report via ECOMP provides a paper trail illustrating the history of the injury in case the employee's condition worsens and he/she decides to formally file a claim.
6.11.11 Injured employee claims shall be filed electronically using the Web-based DOL ECOMP system, which features automatic e-mail reminders to supervisors and ICS's and ensures quick generation of a case number and fewer delays in adjudication. On rare occasions, it may be necessary and acceptable to file a paper-based claim.
6.11.12 Once an employee (or other individual on his/her behalf) has initiated a claim in ECOMP, the injured employee supervisor receives notification that the form is ready for review.
6.11.13 The supervisor shall complete the Form CA-1 or Form CA-2 in ECOMP within three (3) working days of e-mail notification by the ECOMP system.
6.11.14 ICS's shall assist injured employee supervisors with completion of forms in ECOMP, especially with the use of correct DOL codes (e.g., occupation, type, and source of injury), agency identification, and location of duty station.
6.11.15 ICS's will receive progress tracking information throughout the ECOMP claims process.
6.11.16 After the supervisor signs the form in ECOMP, it is sent to the ICS for final processing.
6.11.17 ECOMP transmits the completed forms and any accompanying downloaded paperwork to the OWCP so that a case number is generated.
6.11.18 The OWCP closely tracks NASA's compliance with FECA statutory timeliness of filing requirements.
6.11.19 Timeliness is determined by the OWCP as part of the adjudication process, regardless of the date of filing.
6.11.20 ICS's and injured employee supervisors shall ensure that the Agency portion of the Form CA-1 or CA-2 is complete and submitted to DOL no more than 10 working days after receiving notice that the form has been initiated by the employee and is ready in ECOMP to be reviewed.
6.11.21 Although employees are responsible for ensuring medical evidence is submitted with claims, ICS's and employee supervisors shall not wait for submittal of supporting evidence by the employee before signing or submitting claim forms to OWCP.
6.11.22 When possible, claims documents shall include supporting information such as medical reports and statements from the employee, the supervisor, and any witnesses.
6.11.23 NASA ICS's shall, in coordination with Safety, the onsite OH medical clinic, and employee supervisors, submit to OWCP all claim-related relevant and probative factual and medical evidence in its possession, as well as evidence it may acquire through investigation or other means. Evidence may be submitted at any time.
6.11.24 NASA ICS's shall complete the Receipt of Notice for CA-1 or CA-2 claims. After the employee signs the original form, a copy of the entire Form CA-1 or CA-2, along with any supporting documentation submitted to OWCP, shall be provided to the employee. A "wet signature" original CA-1 or CA-2 shall be retained by ICS's in the employee case file folder.
6.11.25 ICS's, in coordination with injured-employee supervisors, shall use Form CA-17 to obtain interim medical reports about an employee's fitness for duty.
6.11.26 The Form CA-17 is completed by the employee's physician.
6.11.27 CA-17 forms may be sent to the employee's physician at reasonable intervals but not more than once per week to monitor the employee's medical status and his/her ability to return to light or full duty.
6.11.28 On the Agency's portion of the CA-17 form, a notation of the availability of any light or limited duty shall be made.
6.11.29 To aid in returning an injured employee to suitable employment, the ICS may contact the employee's physician in writing concerning the work limitations imposed by the effects of the injury and possible job assignments. NASA ICS's may not directly contact physicians by telephone or through personal visits. Correspondence sent to and received from an employee's physician shall be uploaded to the employee's case file in ECOMP so that OWCP is aware of this activity.
6.11.30 In accordance with DOL OWCP requirements, NASA Centers shall offer appropriate light or limited duty work for employees' safe and expeditious return to work.
6.11.31 Supervisors of injured employees shall make every effort possible to structure or modify an injured employee's work duties to meet medical limitations and to allow the employee to return to work.
6.11.32 Position descriptions do not need to be modified unless the modification is long term.
6.11.33 An injured employee must accept a reasonable offer of limited duty work that he/she can perform or provide an explanation to OWCP for declining. No further compensation for wage loss is payable once the employee has recovered from the work-related injury to the extent that he or she can perform the duties of the position held at the time of injury, or earn equivalent wages.
6.11.34 If an employee cannot return to the job held at the time of injury due to partial disability from the effects of the work-related injury, but has recovered enough to perform some type of work, he or she must seek work.
6.11.35 If telework is offered by NASA as an alternative to enable the employee to work, a formal telework agreement between the employee and NASA shall be completed, submitted, and approved.
6.11.36 Offers of work suitable for an employee based on his/her medical status and physical limitations shall comply with 20 CFR 10.507 and other appropriate requirements.
6.11.37 When an employee cannot return to work in any capacity due to injury and pay will be lost (or expected to be lost) for more than 3 days, a Form CA-7, Claim for Compensation on Account of Traumatic Injury or Occupational Disease, shall be submitted.
6.11.38 All wage loss claims must be supported by medical evidence of injury-related disability for the period of the claim.
6.11.39 If the employee does not qualify for continuation of pay (for 45 days), a CA-7 form should be completed and filed with the OWCP as soon as pay stops.
6.11.40 A CA-7 form should also be submitted when the employee reaches maximum improvement and claims a schedule award.
6.11.41 If the employee is receiving continuation of pay and will continue to be disabled after 45 days, the form should be filed with OWCP five working days prior to the end of the 45-day period.
6.11.42 The CA-7 also should be used to claim continuing compensation when a previous CA-7 claim has been made. Employees are not required to use sick or annual leave before claiming compensation.
6.12.1 A Form CA-16 is furnished to an employee (i) upon his/her request, (ii) when the employee sustains a work-related traumatic injury that requires an emergency medical examination, emergency medical treatment, or both, or (iii) when issuing the form is a more expeditious method of the employee receiving medical assistance/treatment than NASA's electronically submitting routine claim paperwork (CA-1) via ECOMP to obtain a case number for medical providers to use for billing purposes.
6.12.2 A Form CA-16 cannot be issued unless a notice of injury claim has been or is about to be filed.
6.12.3 A Form CA-16 shall be provided by NASA to the employee within four hours of the time of the notification of injury and/or the request by the employee. If there is no time for NASA to complete a Form CA-16 due to the severity of the employee's injury, medical treatment may be authorized by NASA by telephone with subsequent submittal of the CA-16 within 48 hours to the medical treatment facility where the employee is receiving/received treatment. Telephonic notification to an injured employee's medical provider is accomplished by the same individual at his/her Center who is approved to sign Form CA-16 as the Center's authorizing official in accordance with NASA requirements.
6.12.4 NASA cannot issue a CA-16 more than one week after the occurrence of the claimed injury.
6.12.5 Issuance of Form CA-16 is conducted by each NASA Center/Component Facility "authorizing official."
6.12.6 At NASA, the authorizing official is limited to (in order of signature preference): (i) a Civil Service NASA Center Medical Clinic physician/designated Civil Service nurse, (ii) the Center's Occupational Health Clinic Contracting Officer's Representative/Functional Manager/Technical Monitor, or (iii) the injured employee's supervisor. The individual chosen from this list to sign the CA-16, at any given time, will depend on his/her availability and the need for expediting medical assistance to the employee.
6.12.7 Contractor personnel are not permitted to sign CA-16 forms as an authorizing official since doing so constitutes contractual authority to obligate NASA funds.
6.12.8 If a Center's authorizing official is the Center's Occupational Health Clinic Contracting Officer Representative/Functional Manager/Technical Monitor or the injured employee's supervisor, a consultation with the Center's Occupational Health Clinic Medical Director or primary physician shall be conducted before signing the form and issuing it to the employee.
6.12.9 A Form CA-16 must contain the full name and address of the qualified physician or qualified medical facility authorized to provide service before its issuance to the employee by the authorizing official. Because CA-16 forms are normally only issued in emergency situations (e.g., the employee is going to a hospital emergency room), it is assumed that hospital physicians and hospitals are "qualified."
6.12.10 If the NASA "authorizing official" signing the CA-16 doubts that the injury occurred, or that it is work-related, medical care is authorized but block 6B of the CA-16 form is checked. The CA-16 issuance must not be delayed or hindered for any reasons of doubt.
6.12.11 The employee provides the Form CA-16 (and Form OWCP-1500, if available) to his/her treating physician. A CA-17 may also be provided by NASA to accompany Form CA-16 to ensure the treating physician communicates to NASA the medical status of the employee with respect to returning to work.
6.12.12 Other Form CA-16 information:
a. Blank forms are controlled since they financially obligate NASA for any medical expenses incurred by the employee, even if the case is ultimately denied by DOL.
b. Blank forms are controlled and secured at each Center/Component Facility in a method enabling access by personnel at the onsite Medical Clinic (e.g., Civil Service Physician/Nurse), the Center's onsite Medical Clinic COR, and injured employee supervisors. Maintaining a very small quantity of original blank forms ensures their immediate availability in case of an employee emergency.
c. Blank CA-16 form supplies are provided to the Centers/Component Facilities by a NASA Injury Compensation Specialist or the Agency Federal Workers' Compensation Manager.
d. Blank CA-16 forms cannot be e-mailed or photocopied in quantities and distributed.
e. CA-16 authorizes treatment for 60 days from the date of injury, unless OWCP terminates the authorization sooner. If OWCP denies the case, authorization provided by Form CA-16 is invalid after the date of the denial.
f. CA-16 authorizes payment and treatment and services for office visits and consultations, lab work, hospital services (inpatient included), X-rays, MRIs, CT scans, physical therapy, emergency services (including surgery), and chiropractic services (limited to charges for exams and x-rays to diagnose subluxation of spine and manual manipulation of the spine to correct subluxation found by x-ray). CA-16 does not authorize payment for elective and non-emergency surgery.
6.13.1 Form CA-2 shall be filed within 30 days of NASA's knowledge of the injury.
6.13.2 Any CA-2 claim not submitted within three years will be barred by statutory time limitations unless the employee's immediate superior had actual knowledge of the injury within 30 days of occurrence.
6.13.3 For an employee's death due to disease, time begins to run when the employee's survivor is aware, or reasonably should have been aware, of a causal relationship between the death and the factors of employment.
6.13.4 For CA-2 claims, employees who have retired from NASA may wish to file years after they have left the Agency. ICS's shall request information from the former employee's Center OH medical clinic to determine whether he/she participated in any type of medical surveillance program and include the appropriate documentation with claims submittals. Since former employees' supervisors may no longer be at the Agency, ICS's shall provide any extra assistance to former employees in filing claims.
6.13.5 If submitting a Form CA-2, a Form CA-35 "Evidence Required in Support of a Claim for Occupational Disease" form/checklist shall be provided to employees and submitted with the claims.
6.13.6 For occupational disease or illness cases, COP does not apply. Instead, compensation for lost wages is payable after an initial three-day waiting period in non-paid status. If the disability exceeds 14 days from the time compensation begins, no waiting period is required.
6.14.1 Determinations that set forth OWCP's findings in a case and includes a description of the employee's appeal rights is known as a formal decision and are sent to the employee by the OWCP in writing.
6.14.2 OWCP issues a formal decision whenever it reaches an adverse decision about entitlement, such as denial of an initial claim or denial of continuing benefits.
6.14.3 Three avenues of appeal are provided for employees (NASA is not entitled to appeal), and the employee may request only one form of appeal at a time.
6.14.4 Employees are entitled to either an oral hearing before an OWCP representative or a review of the written record (but not both), as long as a request in writing is made within 30 days of the formal decision and a reconsideration has not already been requested. Hearings may be held in person (within 100 miles of the employee's home), by telephone, or video conference at the discretion of the hearing representative. If the hearing is held in person, the employee may present written evidence or oral testimony in support of the case. If a review of the written record is chosen, the employee may not present oral testimony but he or she may submit written evidence or argument.
6.14.5 If an oral hearing is requested, OWCP will advise NASA of the date and time. NASA may have one representative (or more when needed) present at the hearing and/or request a copy of the transcript. NASA may not participate in the proceedings unless specifically invited to do so by the employee or the OWCP representative. For either an oral hearing or a review of the written record, OWCP will allow NASA 20 days to submit comments and/or additional documents, which will be subject to review and comment by the employee within a further 20 day period. After the oral hearing is held or the review of the written record is completed, OWCP will issue a formal decision, including a description of the employee's further appeal rights.
6.14.6 The employee may ask OWCP to reconsider a formal decision made by the district office, stating the grounds on which it is based and accompanied by relevant evidence not previously submitted or arguments for error in fact or law in reaching the contested decision. Reconsideration must be requested within one year of the date the contested formal decision was issued. OWCP will provide NASA with a copy of the employee's request and allow 20 days for submittal of comments and/or documents which will subsequently be subject to the employee's review and comment within 20 days. Following reconsideration, OWCP will issue a new formal decision that includes a description of the employee's further appeal rights.
6.14.7 An employee may request review by the Employees' Compensation Appeals Board (ECAB), which is the highest authority in Federal Workers' Compensation claims. The request is filed directly with the ECAB within 180 days of the date of the decision. The ECAB's review is based solely upon the case record at the time of the formal decision; new evidence is not considered.
7.1.1 To fulfill its mission, the OCHMO defines OH "requirements" as mandatory elements for programs or functions. Periodic Agency Occupational Health (OH) reviews are conducted to ensure adequate programs are implemented at the Centers, and ultimately to protect and promote NASA workforce health, improve workers' capabilities and abilities, and ensure the maintenance of their safe and healthy working environment. Centers are required to conduct annual self-assessments to ensure maintenance of program quality during the two years between Agency OH review team onsite reviews.
7.1.2 Requirements include NASA Policy Directives (NPDs), NPRs, and external Federal, state, and local regulations and consensus standards applicable to NASA.
7.1.3 This chapter establishes:
a. Criteria for performing and documenting the results of, and delineating the requirements for, Agency periodic OH reviews conducted at all NASA Centers, including NASA Headquarters (HQ) and NASA's Jet Propulsion Laboratory to the extent required in their contract.
b. Criteria for performing and documenting the results of, and delineating the requirements for, Center annual OH reviews conducted at NASA Centers, including NASA HQ and NASA's Jet Propulsion Laboratory to the extent required in their contract.
7.2.1 All OH program reviews and self-reviews shall:
a. Identify and mitigate health risk;
b. Ensure provision of consistent, high-level health care;
c. Identify best practices and innovative solutions that provide greater operational effectiveness and efficiency;
d. Assess the adequacy of resources commensurate with the Center's size, population, and mission; and
e. Include assessment of:
(1) Medical care provided at each Center's Occupational Medicine clinic (including emergency care capability and coordination with other departments, medical quality assurance, health clinic environment of care, childcare facility health aspects, and preventive health and wellness activities);
(2) Employee Assistance Programs;
(3) Federal Workers' Compensation Program Case Management (JSC & NSSC);
(4) Fitness Program and Facilities
NOTE: NASA component facility fitness clubs or similar exercise clubs that utilize equipment and/or other accessories within NASA-maintained interior space shall be reviewed triennially but on a limited basis with written recommendations for improvements (if any) provided to the appropriate component facility management and stakeholders.
(5) Industrial Hygiene Programs;
(6) Health Physics and Radiation Safety Programs; and
(7) Food Safety Programs.
7.2.2 OH review and self-review team members shall be qualified to conduct reviews in their respective program areas per NPD 1210.2, NASA Surveys, Audits, and Reviews Policy.
7.2.3 All OH reviews and self-reviews shall compare NASA Center policies, procedures, and practices to OH requirements, as defined in this NPR.
7.2.4 All OH review and self-review findings shall be categorized as follows:
a. Commendation: A practice that exceeds requirements, is an Agency best practice, or is a time or cost-saving measure, that occurs without sacrificing OH objectives or requirements;
b. Recognition: The acknowledgement of a significant improvement or progress toward meeting Center OH program requirements or other positive noteworthy accomplishment. While not attaining levels commensurate with those of a commendation — it is still worthy of acknowledgement;
c. Opportunity for Improvement: A condition that could or should be improved. Opportunities for Improvement (OFI's) are accompanied by "Recommendations" in the written report. Recommendations are not "required" to have Corrective Action Plans (CAPs) in the Surveys, Audits, and Assessments Information System (SAARIS) unless specifically requested by the OH review team lead. Centers shall suitably address OFI's within their internal action processes;
d. Nonconformance: A divergence from a requirement (Federal, state, local, NASA Agency, NASA Center, etc.) or an applicable consensus standard (ANSI, NIOSH, etc.) that may cause undue risk. These findings require Center response in the form of a Corrective Action Plan in SAARIS, along with follow-on status reports in SAARIS; and
e. Observation: Observations can be external or internal. An External Observation is defined as a neutral (non-positive and non-negative), informational comment to the Center. An Internal Observation is defined as a reviewer comment, either for the record or to help the reviewer in future reviews.
7.2.5 All OH review and self-review working documents, reports, and other information and data shall be retained on file or in the Agency EHRS in accordance with NASA's record requirements and this NPR.
7.3.1 In addition to the provisions for reviews provided in section 7.2 of this chapter, Agency OH reviews shall:
a. Provide a forum for NASA Center/Facility personnel and OH review team to discuss OH-related issues; and
b. Provide advocacy for the Centers'/Facilities' occupational health disciplines by offering technical help, guidance on best practices, support for Agency OH initiatives, facilitation of specialized training for emerging health threats and new requirements, and enhancement of the competency of OH employees.
7.3.2 The latest review schedule shall be maintained on the Agency OH Web site.
NOTE: Additional responsibilities for Agency OH reviews are delineated in Table 1.
7.4.1 The CHMO shall ensure that periodic OH program reviews of NASA Centers are conducted, final OH reports are reviewed and approved, and results provided to Center Directors.
7.4.2 Centers shall:
a. Appoint a Center POC, with sufficient authority and OH knowledge, to coordinate Agency OH onsite reviews with the Agency OH review lead and provide ready access to facilities and other logistical support;
b. Ensure that adequate and professionally appropriate technical points of contact for each OH program are available to participate in the OH review for the entire review period;
c. Support the OH review team with adequate resources and personnel;
d. Provide comprehensive answers and relevant information on the discipline-specific questionnaires;
e. Make all pertinent records, documentation, and information available to the Agency OH Review Team for review and assessment in a timely manner;
f. Provide for a management representative, familiar with Center OH operations, to attend the Agency OH review in-briefing, or specify an alternate, that is familiar with Center OH operations, if he/she is unavailable;
g. Provide for a senior management representative to attend the Agency OH review out-briefing, or specify an alternate if he/she is unavailable;
h. Ensure that final OH self-review reports are reviewed and approved, and the results provided to Center Directors;
i. Ensure corrective action plans for all nonconformance findings are developed and entered into the SAARIS according to Table 1 specifications so OCHMO and the Center OH Office can validate remediation has been completed; and
j. Provide adequate resources to resolve corrective actions.
7.4.3 The Center POC shall be responsible for:
a. Coordinating and exchanging information with the Agency OH review team leader which includes:
(1) Providing a discipline-specific POC list, including names, mail and e-mail addresses, and phone numbers at or before the designated due date.
(2) Distributing review questionnaires to Center personnel.
(3) Validating and providing completed questionnaires and requested documentation at or before the due date, and in the designated electronic folder format.
b. Providing and coordinating support requirements as noted on the "request for support" document;
c. Using SAARIS to enter their Corrective Action Plans and other pertinent review information;
d. Tracking corrective actions to closure in SAARIS;
e. Downloading and distributing the OH discipline-specific questionnaires and request for documents to the appropriate Centers' OH representatives; and
f. Supporting the Agency OH review team.
7.4.4 Center discipline-specific points of contact shall be responsible for:
a. Being available during all parts of the review for their OH review team counterparts;
b. Coordinating and exchanging OH discipline information with the appropriate OH review team counterpart;
c. Providing objective evidence (e.g., documentation, all necessary records, licenses, etc.) as requested;
d. Reporting real-time issues, problems, and findings status to their Center POC, as they arise, during the review process;
e. Escorting Agency OH review team personnel;
f. Coordinating and verifying with their discipline specific Agency OH review team counterparts all specific discipline findings prior to the informal out-briefing;
g. Supporting the development of corrective action plans for each nonconformance finding; and
h. Representing their Center at the Agency OH review in-briefing, Agency OH informal out-briefings, and Agency OH senior management out-briefing.
7.5.1 In addition to the requirements of this section, Agency OH reviews shall follow the provisions of section 7.2 of this Chapter.
7.5.2 Agency-level OH reviews of NASA Centers are conducted by the Agency OH review team periodically.
7.5.3 Periodic reviews are scheduled in advance by the Agency OH review team and are conducted (to the greatest extent possible) during the same month at each respective Center during the target year.
7.5.4 Center POCs shall download (from the OHP Web site) and distribute the OH discipline-specific questionnaires and request for documents to the appropriate Centers' OH representatives, and support the OH review team.
7.5.5 Answers to questionnaires shall be all inclusive and representative of all Center contractor and NASA activities.
7.5.6 The Centers' POC shall review the Center-completed questionnaires and determine their viability, prior to returning them to the Agency OH review team.
7.5.7 Concurrently with submitting the questionnaires and documents requested, the Center POC shall also provide the Agency OH review team with:
a. A list of the technical Center POC's for each OH discipline;
b. Center security requirements;
c. In-brief and out-brief locations, including building numbers and/or names, and room numbers; and
d. Other logistical information as needed for the Agency OH review.
7.5.8. All requested information shall be compiled in the Agency OH review team file folder format specified in the e-mail sent to the POC in accordance with the timeline in Table 1.
7.5.9 The Agency OH review shall include an in-briefing as requested in the e-mail to the POC and in the letter to the Center Director. The in-briefing agenda and time shall be specified in the letter to the Center Director after coordination with the POC.
7.5.10 A written and/or electronic listing of all nonconformance findings will be provided to the Center at the time of the senior management out-briefing.
7.5.11 The out-briefing shall be presented by the Agency OH review team to the Center Director or his or her senior management representative in a verbal, executive summary format for each discipline.
7.5.12 A report shall be prepared by the Agency OH review team based on the review findings.
7.5.13 The report shall be a reiteration of the issues expressed in the Center senior management
out-briefing and shall additionally include details of all review findings.
7.5.14 The report shall consist of a cover letter, an executive summary with a table of findings by type of finding and functional category, and the detailed audit card findings.
7.5.15 Centers shall track and close all nonconformance findings using the SAARIS.
7.5.16 Centers shall not submit written CAP status updates to the Agency OH review team.
7.5.17 Table 1 summarizes the tasks and associated timelines and requirements for the Agency OH review process.
Table 1
Timeline and Requirements for the OH Review Process
| Task | Timeline | Responsible Organization/Party | |
|---|---|---|---|
| 1 | Memo to Center Directors with annual OH review schedule for upcoming year | By November 1 of the previous year | Agency OH review team |
| 2 | Electronic communication to Center POC with a request for documents for the Agency OH review NOTE: Documents are available from the OHP Web site |
Approximately 120 days before the Agency OH review visit is scheduled to take place at the Center | Agency OH review team |
| 3 | Center-completes OH review, questionnaires, assembles requested documents, and discipline-specific POC information and provides them to the Agency OH review team | 60 days or more before the Agency OH review takes place; or by the due date indicated in the Agency OH review team's previous communication | Center POC |
| 4 | Notification of the Center Director of the upcoming OH review | Approximately 30 days before Agency OH review visit is scheduled to take place at the Center | Agency OH review team |
| 5 | Listing of nonconformance findings is provided to the Center | Senior Management Out-brief | Agency OH review team |
| 6 | Memo and Executive Summary report sent to Center Director with the results of the OH review; An electronic copy with detailed audit card findings distributed electronically to Center Director, Center POC, the appropriate Mission Associate Administrator, Institutional Corporate Management, and Safety and Mission Assurance Directorates | Approximately 60 days after the last day of the Agency OH review | Agency OH review team |
| 7 | Corrective Action Plans for nonconformance findings due in SAARIS | 6 months after the last day of the Agency OH review | Center POC |
| 8 | Review implementation status of CAPs | By the next triennial Agency OH review of the Center | Agency OH review team |
7.5.18 Immediately dangerous to life and health (IDLH) situations found by the Agency OH review team shall be addressed as follows:
a. The Agency OH review team member shall endeavor to keep personnel from exposure to any IDLH situation and shall immediately report the matter to an onsite Center representative directly (if present), by phone, or other means.
b. As soon as practicable, the Agency OH review team member shall report the matter to the Agency Review Team Leader and Center Team Leader.
c. The Agency reviewer shall not commence the review until the issue has been resolved and the condition is no longer IDLH.
7.6.1 Center self-reviews shall be comparable to Agency OH reviews in profundity, quality, and efficacy.
7.6.2 Centers shall perform annual Center OH self-reviews during years when Agency OH reviews are not performed.
7.6.3 In addition to the requirements of this paragraph, Center self-reviews shall follow the provisions of section 7.2 of this Chapter.
7.6.4 Centers shall ensure corrective action plans for all nonconformance findings are developed and entered into SAARIS.
7.6.5 Self-reviews may be conducted anytime, but results and products shall be completed and findings with supporting documentation entered into SAARIS, as per the requirements in Table 2, Timeline for Center Self-Reviews.
7.6.6 Centers shall prepare a written report based on their OH review findings for their Center Director and appropriate senior managers.
7.6.7 The report shall consist of a memo, executive summary, and detailed findings by functional categories.
7.6.8 Centers shall use the most current self-evaluation tools and instructions, which are provided on the Agency OHP Web site to conduct self-reviews.
7.6.9 Conducting a Center OH self-review shall include:
a. A self-assessment performed against the requirements of NPR 1800.1, using the Agency OH questionnaires as a guidance tool;
NOTE: Questionnaires may be found on the Agency OH Web site. If the Agency OH questionnaires are not used, the Center must use another questionnaire or appropriate tool to ensure all program elements are reviewed and provide to OCHMO upon request. Submission of completed questionnaires to OCHMO is not required.
b. A self-assessment performed on the Center's records and documents. Submission of the list of Center documents assessed as part of the self-review is required;
NOTE: This is based on the list of the "Request for Documents and Information" found on the OHP Web site. Submission of the actual records and documentation is not required.
c. An assessment and status update of any of the Center's open nonconformance findings from previous Agency OH reviews and/or Center OH self-reviews. Submission of the list and status of open nonconformance findings is required;
d. A list of individuals, by disciplines, who performed or were involved in the Center OH self- review. The listing shall include their professional qualifications relative to the self-review. Submission of the list of individuals and their qualifications is required;
e. A list of areas, by discipline, that were reviewed as part of the self-review. Submission of the list of areas reviewed is required;
f. A list of the individuals, by discipline, who were interviewed as part of the self-review. Submission of the list of individuals interviewed is required; and
g. Any substantial changes, positive or negative in each OH Program discipline. Submission of the substantial changes is required.
7.6.10 The non-submittal of an OH self-review from the Center during an off-year shall be referred to the CHMO for decision on further action and reflected in the Center's subsequent onsite Agency OH Review detailed report.
NOTE: Additional requirements for Center OH review teams are delineated in Table 2.
Table 2: Timeline and Requirements for Center Self-Reviews
| Task | Timeline | Responsible Organization/Party |
|---|---|---|
| Conduct off-year OH self-reviews and record findings in SAARIS with supporting documentation and status of previous nonconformance findings | On or before December 31st of each year | Center OH POC |
| Annually submit information and send to the SEHO (or designee) in support of the Annual OSHA Report* | On or before December 31st of each year | Center OH and Safety POC |
*NOTE: Although not directly part of the OH review process, the additional information is closely related to Center self-reviews. Centers should consider doing self-reviews and information gathering in support of the Annual OSHA Report simultaneously.
Action Level, Noise. An 8-hour time-weighted average of 82 decibels measured on the A-scale, slow response, or equivalently, a dose of 50 percent. Employee exposure at or above the action level shall trigger enrollment into a hearing conservation program.
Active Managerial Control. The purposeful incorporation of specific actions or procedures by management into the operation of their establishment to attain control over risk factors.
Administrative Control. Any procedure that limits exposures through the restriction of area access, exposure times, distance, and/or work practices.
As Low As Is Reasonably Achievable (ALARA). As defined in Title 10, Section 20.1003, of the Code of Federal Regulations (10 CFR 20.1003), ALARA means making every reasonable effort to maintain exposures to ionizing radiation as far below the dose limits as practical, consistent with the purpose for which the licensed activity is undertaken, taking into account the state of technology, the economics of improvements in relation to state of technology, the economics of improvements in relation to benefits to the public health and safety, and other societal and socioeconomic considerations, and in relation to utilization of nuclear energy and licensed materials in the public interest
As Low As Is Reasonable Practicable (ALARP). ALARP means making every reasonable effort to maintain exposures (other than to ionizing radiation) as low as practicable, consistent with budgetary and operational constraints. In no case shall ALARP levels exceed legal or consensus OELs.
Audiometer. An electronic instrument used for measuring hearing threshold levels that conforms to the requirements and specification of the current American National Standard Institute (ANSI) S3.6, Specification for Audiometers standard.
Baseline Audiogram. The reference audiogram against which future audiograms are compared, typically resulting from an audiometric evaluation conducted at the time the employee is enrolled in the hearing conservation program.
Biological Agents. Pathogenic bacteria, viruses, fungi, and other microorganisms and their associated toxins that have the ability to adversely affect human health in a variety of ways, ranging from relatively mild, allergic reactions to serious medical conditions, and death.
"Buy Quiet and Quiet by Design" Programs. Site-specific programs that endeavor to achieve long-term reduction of employee noise exposures through purchase and design of equipment that meet realistic and achievable noise-emission criteria, which are considered before procurement or design. The "Buy Quiet and Quiet by Design" approach requires designers and engineers to consider noise emission when purchasing and designing equipment that is expected to generate noise emission levels of concern for hearing conservation (80 dBA and higher).
Calibration. A check of proper functioning and stability of a measurement instrument by various means. In cases where methods or requirements vary, the methodology or specification that results in the most accurate data collection shall apply.
Competent Person. OSHA defines competent person as "one who is capable of identifying existing and predictable hazards in the surroundings or working conditions which are unsanitary, hazardous, or dangerous to employees, and who has authorization to take prompt corrective measures to eliminate them".
Cottage Foods. State defined but in general, non-time-temperature control for safety foods such as baked goods, jams, and jellies produced at a cottage food operation. Acidified foods, low-acid canned foods, garlic in oil, and fresh fruit or vegetable juices are examples of foods that present a food safety risk and may not be produced at a cottage food operation. NOTE: Cottage food laws vary by state and some may be less or more restrictive than defined here. Centers should follow the most restrictive requirements.
Cottage Food Vendor. State defined but in general, a person who produces cottage foods in the home kitchen of their primary domestic residence and only for sale directly to the consumer. A cottage food operation is not permitted to operate as a food service establishment, retail food store, or wholesale food manufacturer.
Criterion Sound Level. A Time Weighted Average (TWA) occupational noise exposure level, expressed in decibels on the A-weighted scale (DVA) with a decibel (dB) exchange rate. NASA's criterion sound level, or 100% dose, is the equivalent of 85 dBA, 8-hour TWA, with a 3 dB exchange rate, as shown in Table 2 of the document.
Critical Incident Stress Management: The constellation of services or activities that may be used by an organization to respond to and manage a critical incident. Services and activities include, but are not limited to, debriefings, outreach to the workforce, psycho-educational activities related to trauma, anniversary responses, etc.
Decibel A-weighted (dBA). A sound level reading in decibels made on the A-weighted network of a Sound Level Meter (SLM) at slow response.
Decibels, Peak (dBP). The highest instantaneous sound level measured. Commonly used to measure impulsive or impact noise. This quantity cannot be measured on the slow response A-weighted scale and is usually measured on the C-weighted scale.
De-rating. The process of reassigning the manufacturers' values of hearing protectors to more realistic, real-world performance values.
Design Review. A formal documented and systematic examination of a design to evaluate facilities and/or operations relative to health, safety and other aspects.
Developmental Toxicity. Adverse effects on the developing organism that may occur anytime from conception to sexual maturity and include such effects as spontaneous abortion, structural or functional defects, low birth weight, or effects that may appear later in life.
Dose. The amount of any given substance absorbed by the body (including radiation and other energies).
Drug Free Workplace. Laws, regulations and policies emanating from Executive Order (EO) 12564 of September 15, 1986, and subsequently the Drug-Free Workplace Act of 1988, that ordered federal employees to refrain from using illegal drugs, whether on or off duty. It mandates that the head of each Executive agency shall develop a plan for achieving the objective of a drug-free workplace. Elements of the plan include establishing a program to test for the use of illegal drugs by employees in sensitive positions; training for managers and employees; and establishment of EAPs that emphasize high-level direction, education, counseling, referral to rehabilitation, and coordination with available community resources.
EAP Model. Refers to the method of delivering EAP services. The types of services offered through the EAP may vary but are typically delivered through a model such as:
1. Internal model, where the EAP staff is comprised of federal employees and there are no contractors involved.
2. External model, where the sponsoring federal agency has entered into a contract for an outside vendor to provide all EAP-related services.
3. Blended model, where both federal and contract personnel are involved in the delivery of
EAP services. The federal employees usually have the role of monitoring the EAP contractor's services, billing, and performance, while also providing counseling and other administrative services.
4. Consortium model, where a group of federal agencies contracting with one agency or
contractor to provide employee assistance services.
Employee Assistance Program (EAP). An EAP is a worksite-based program designed to assist in the identification and resolution of work-related and non-work-related productivity problems associated with employees impaired by personal concerns including, but not limited to, health, marital, family, financial, alcohol, drug, legal, emotional, or other personal concerns which may adversely affect employee job performance. The specific core activities of EAPs include (1) services for individuals (such as identification and resolution of job-performance issues related to an employee's personal concerns, and assessment, referral, and follow-up); (2) services for managers and supervisors (such as assistance in referring employees to the EAP, supervisor training, and management consulting); (3) services for organizations (such as violence prevention/crisis management, group interventions, and employee orientation); and (4) administrative services (such as the development of EAP policies and procedures, outreach, evaluation, and referral resources development).
Employer. NASA organizations and their associated contractors, to the extent specified in their respective contracts, and other Government agencies, their contractors, and tenants whose primary work is performed at a NASA Center.
Engineering Control. Any mechanical device or physical barrier that reduces the magnitude of an exposure along the path of propagation to the potentially exposed individual. Engineering controls should be employed first and do not include personal protective equipment or administrative controls.
Exchange Rate, Noise. The increase or decrease in decibels corresponding to twice (or half) the noise dose. When using a 3 dB exchange rate, a dose corresponding to an exposure of 85 dBA, 8-hour TWA represents twice the dose associated with an 82 dBA, 8-hour TWA exposure.
Farmers Market. A public and recurring assembly of farmers or their representatives (produce vendors) and cottage food vendors selling the food that they produced directly to consumers.
Farmers Market Vendor. An individual farmer or farmer's representative (produce vendor) or cottage food vendor who participates in farmers markets held onsite at NASA Centers through a signed agreement with the Center Market Manager.
Food Manager Certification. A written certification test that requires food managers to demonstrate a basic knowledge of food protection practices.
Food Safety Inspectors. Persons who have received specific training, and certification or standardization in the area of food inspection and regulations from an agency that regulates the food industry, or has been credentialed by a state or the National Environmental Health Association.
Functional Ability Evaluations. Evaluations performed for the purpose of determining a worker's ability to perform specific job tasks (ability) and job demands. Also includes the processes used to evaluate the ability of individuals to safely perform essential duties, if placed in a noisy work environment.
Hazard. A biological, physical, or chemical property that may cause an unsafe condition.
Hazard Analysis Critical Control Point (HACCP) Methodology. A prevention-based food safety management system that identifies and monitors specific food safety hazards that can adversely affect the safety of food products.
Hazardous Noise Area. Any work area where the environmental noise level is at or above 85 dBA, or where the environmental impulse noise level is at or above 140 dBC peak or linear, regardless of duration of exposure or number of impulses.
Hazardous Substance or Article. Any material, object, or agent that, because of its quantity, concentration, physical, chemical, infectious, radioactive, or toxic properties poses a significant present or potential hazard to human health and safety by its misuse or if released into the workplace or the environment.
Hearing Threshold Level (HTL). The hearing level, above a reference value (audiometric zero), at which a specified sound or tone is heard by an ear in a specified fraction of the trials. For pure-tone air-conduction audiometry, hearing levels are sound pressure levels of pure tones at audiometric frequencies, such that 0 dB HTL, or audiometric zero, typifies the threshold of hearing of young ontologically-normal persons.
Impulsive or Impact Noise. Variations in noise levels that involve peaks of intensity that occur at intervals of greater than 1 second. If the noise peaks occur at intervals of 1 second or less, the noise is considered continuous.
Major Food Safety Incident. Any of the following or related events occurring at an establishment at NASA facilities on NASA property: a known poisoning resulting in hospitalization; two or more suspected poisonings; any known or suspected incident of food contamination resulting or potentially resulting in exposure to personnel; or any similar or related incidents. All major food safety incidents will be categorized and investigated based on NPR 8621.1, NASA Procedural Requirements for Mishap and Close Call Reporting, Investigating, and Recordkeeping.
Market Manager. A NASA civil service or contract (per the contractor's contract) employee responsible for operation of the farmers market, including vetting farmers market vendors to ensure they meet NASA's requirements for selling food at the market and working with the Food Safety Inspector to help farmers market vendors understand NASA food safety requirements and correct deficiencies noted during inspections.
Maximal medical improvement. A condition or state that is well stabilized and unlikely to change substantially in the next year, with or without medical treatment. Over time, there may be some change; however, further recovery or deterioration is not anticipated.
Nanoparticles. Materials that have at least one dimension (e.g., length, width, height, diameter) that is less than 100 nanometers. Nanoparticles may be suspended in a gas (e.g., nanoaerosol), suspended in a liquid (e.g., nanocolloid or nanohydrosol), or embedded in a matrix (e.g., nanocomposite).
Nanometer (nm). 1 x 10-9 meters or one millionth of a millimeter.
Noise Dose. A measure of cumulative noise exposure over a stated time period, which takes into account both the intensity of sound and the duration of exposure. Dose is a dimensionless quantity that represents the amount of actual noise exposure relative to the amount of allowable noise exposure (criterion level) and for which 100 percent and above represents noise exposures that are hazardous.
Noise Dosimeter. An instrument that integrates a function of sound pressure over a period of time in such a manner that it directly indicates a noise dose.
Noise Reduction Rating (NRR). A noise reduction value, in decibels, averaged across the frequencies from 125 Hz to 8 kHz and computed from laboratory tests of the attenuation of hearing protectors measured under ideal conditions. The NRR, per a 1979 Environmental Protection Agency (EPA) regulation, is required to appear on all devices worn on the head or ear that are sold for purposes of personal noise reduction. See "De-rating."
Noise Survey. A periodic or event-driven measurement of sound in areas where exposure to the sound level is likely to be hazardous.
Occupational Hearing Conservationist (OHC). Also known as an industrial audiometric technician. A person who is certified by the Council on Accreditation for Occupational Hearing Conservation (CAOHC) and conducts the practice of hearing conservation, including pure-tone air-conduction hearing testing and other associated duties under the supervision of an audiologist or physician.
Packaged Food. Food that is labeled in accordance with federal, state, and local regulations, and the FDA Food Code. Proper labeling includes name of manufacturer and an accurate statement of the contents.
Pests. Any of various small animals or insects that are destructive or pose a health hazard to humans, plants, or animals in the environment.
Potentially Hazardous Food. A food, natural or synthetic, that requires temperature control because it is capable of supporting the rapid and progressive growth of infectious or toxigenic microorganisms.
Produce. Fruits and vegetables grown for human consumption.
Representative Exposure, Noise. Measurements of an employee's noise dose or 8-hour time-weighted average sound level that is representative of the exposure of other employees exposed to the same noise hazard.
Requirement. NASA Policy Directives (NPDs), NASA Procedural Requirements (NPRs) and external federal, state and local regulations and consensus standards applicable to NASA.
Reproductive Toxicity. Adverse effects on the health of the reproductive organs, endocrine system, or gametes (egg or sperm) from exposure to an exogenous agent that may result in effects such as menstrual dysfunction, impaired fertility, feminization/masculinization, or inability to maintain a pregnancy.
Retail Food Establishment. Any operation, with the exception of Farmers Markets, including childcare and NASA Exchange-operated facilities, that stores, prepares, packages, vends, or otherwise provides food for human consumption at NASA facilities or on NASA property and required to follow all the food safety requirements contained in this document.
Revised Baseline, Hearing Conservation. The most recent audiogram that has established a persistent STS or a significant improvement upon retest.
Risk-Based Inspection, Food Safety. An assessment of the degree of active managerial control that an operator has over the foodborne illness risk factors in the establishment; and the focusing of inspections on the control of foodborne illness risk factors, which embody a preventive rather than reactive approach to food safety.
Risk Factor, Food Safety. One of the broad categories of contributing factors to foodborne illness outbreaks, as identified in the Centers for Disease Control and Prevention (CDC) Surveillance Report for 1993-1997. This report directly relates to foodborne safety concerns within retail and food service establishments. Food risk factors are: Food from Unsafe Sources, Inadequate Cooking Temperatures, Improper Holding Temperatures, Contaminated Equipment, and Poor Personal Hygiene.
Significant Improvement, Hearing Conservation. A significant improvement is shown if the average of thresholds at 2000, 3000, and 4000 Hz for either ear shows an improvement of 5 dB or more from the baseline audiogram.
Sound Pressure Level (SPL). 20 times the common logarithm of the ratio of the square of the measured A-weighted sound pressure to the square of the standard reference pressure of 20 micropascals.
Standard Threshold Shift (STS). A decline in hearing threshold, relative to the baseline audiogram, of an average of 10 dB or more at 2000, 3000, and 4000 Hz in either ear.
Temporary Event, Food Safety. A food establishment that operates in conjunction with a single event or celebration.
Time/Temperature Control for Safety Food. A food that requires time/temperature control for safety to limit pathogenic microorganism growth or toxin formation.
Vector. An organism that is capable of transmitting a pathogen from one organism to another.
Work Role Position. Any job or function, held by a person at a NASA Center that does not change appreciably when a contract is awarded to a new contractor.
| Acronym/Abbreviation | Name for Acronym/Abbreviation |
|---|---|
| ABIH | American Board of Industrial Hygiene |
| ABSL | Animal Biosafety Level |
| ACGIH | American Conference of Governmental Industrial Hygienists |
| ACS | American Cancer Society |
| ACSM | American College of Sports Medicine |
| AED | Automatic External Defibrillator |
| AIHA | American Industrial Hygiene Association |
| ALARA | As Low As Reasonably Achievable |
| ALARP | As Low As Reasonably Practicable |
| ALS | Advanced Life Support |
| ALT | Alanine Transaminase |
| AME | Aviation Medical Examiner |
| ANSI | American National Standards Institute |
| ASHRAE | American Society of Heating, Refrigeration, and Air Conditioning Engineers |
| ASME | American Society of Mechanical Engineers |
| ATSDR | Agency for Toxic Substances and Disease Registry |
| BBP | Bloodborne Pathogen |
| Be-LPT | Beryllium Lymphocyte Proliferation Test |
| BMBL | Biosafety in Microbiological and Biomedical Laboratories |
| BMI | Body Mass Index |
| BP | Blood Pressure |
| BSC | Biological Safety Cabinet |
| BSL | Biosafety Level |
| BUN | Blood Urea Nitrogen |
| B2-M | Beta-2 Microglobulin in Urine |
| CAOHC | Council for Accreditation in Occupational Hearing Conservation |
| CBC | Complete Blood Count |
| CCHO | Certified Chemical Hygiene Officer |
| CCP | Critical Control Point |
| CdB | Cadmium in Blood |
| CDC | Center for Disease Control |
| CdU | Cadmium Urine |
| CFR | Code of Federal Regulations |
| CHMM | Certified Hazardous Materials Manager |
| CHMO | Chief Health and Medical Officer |
| CHP | Certified Health Physicist |
| CIH | Certified Industrial Hygienist |
| CISD | Critical Incident Stress Debriefing |
| CISM | Critical Incident Stress Management |
| CL | Critical Limit |
| CLIA | Clinical Laboratory Improvement Amendments |
| CLSO | Certified Laser Safety Officer |
| CNS | Central Nervous System |
| COOP | Continuity of Operations Plan |
| COP | Continuation of Pay |
| COR | Contracting Officer Representative |
| COTS | Commercial Off-the-Shelf |
| CV | Cardiovascular |
| DASHO | Designated Agency Safety and Health Official |
| dB | Decibel |
| DFWP | Drug-Free Workplace Program |
| DHHS | Department of Health and Human Services |
| DNA | Deoxyribonucleic Acid |
| DOD | Department of Defense |
| DOE | Department of Energy |
| DOL | Department of Labor |
| DOT | Department of Transportation |
| EAP | Employee Assistance Program |
| ECG | Electrocardiograph |
| ECOMP | Employees Compensation Operations Management Portal |
| EH | Environmental Health |
| EHO | Environmental Health Officer |
| EHRS | Electronic Health Record System |
| EMS | Emergency Medical Services |
| EP | Emergency Preparedness |
| EPA | Environmental Protection Agency |
| FAA | Federal Aviation Administration |
| FAR | Federal Acquisition Regulations |
| FC | Fitness Center |
| FDA | Food and Drug Administration |
| FECA | Federal Employees Compensation Act |
| FEHP | Federal Employee Health Program |
| FEHBP | Federal Employee Health Benefits Program |
| FEV 1 | Forced Expiratory Volume in the 1st Second |
| FFD | Fitness For Duty |
| FS | Food Safety |
| FSIO | Food Safety Inspection Officer |
| FVC | Forced Vital Capacity |
| FWC | Federal Workers' Compensation |
| g or gm | Gram |
| GI | Gastro Intestinal |
| GXT | Graded Exercise Test |
| HA | Hazard Assessment |
| HACCP | Hazard Analysis Critical Control Point |
| HazMat | Hazardous Materials |
| HCP | Hearing Conservation Program |
| HCT, Hct | Hematocrit |
| HDL | High Density Lipoprotein |
| HgB | Hemoglobin |
| HHS | Health and Human Services |
| HIMS | Health Information Management System |
| HIPAA | Health Insurance Portability and Accountability Act |
| HIV | Human Immunodeficiency Virus |
| HMTA | Health and Medical Technical Authority |
| HP | Health Physics |
| HPD | Hearing Protection Device |
| HPW | Health Promotion Workgroup |
| HQ | Headquarters |
| HRA | Health Risk Assessment |
| HRO | Human Resource Office |
| HTL | Hearing Threshold Level |
| HVAC | Heating, Ventilation and Air Conditioning |
| Hz | Hertz |
| IAQ | Indoor Air Quality |
| ICC | Infection Control Committee |
| ICISF | International Critical Incident Stress Foundation |
| ICO | Infection Control Officer |
| ICP | Infection Control Plan |
| IDLH | Immediately Dangerous to Life and Health |
| IEEE | The Institute of Electrical and Electronics Engineers |
| IH | Industrial Hygiene |
| IPM | Integrated Pest Management |
| JHA | Job Hazard Analysis |
| JPL | Jet Propulsion Laboratory |
| JSA | Job Safety Analysis |
| JSC | Johnson Space Center |
| KSC | Kennedy Space Center |
| LDL | Low Density Lipoprotein |
| LSC | Laser Safety Committee |
| LSO | Laser Safety Officer |
| LSRB | Laser Safety Review Board |
| MBOCA | 4,4'-Methylenebis(2-chloroaniline) |
| MC | Methylene Chloride |
| MCH | Mean Corpuscular Hemoglobin |
| MCHC | Mean Corpuscular Hemoglobin Concentration |
| MCV | Mean Corpuscular Volume |
| MDA 4,4 | Methylene Dianiline |
| MDI | Methylene Diphenyl Isocyanate or Methylene Diisocyanate |
| mL | Milliliter |
| MMR | Measles, Mumps and Rubella |
| MOCA | 4,4'-Methylenebis(2-chloroaniline) |
| MPEL | Maximum Permissible Exposure Limit |
| MRO | Medical Review Officer |
| MSD | Musculoskeletal Disorder |
| MWT | Maximum Work Times |
| NASA | National Aeronautics and Space Administration |
| NCRP | National Council on Radiation Protection |
| NFPA | National Fire Protection Association |
| NIH | National Institutes of Health |
| NIOSH | National Institute for Occupational Safety and Health |
| NIST | National Institute of Standards and Technology |
| NPD | NASA Policy Directive |
| NPR | NASA Procedural Requirements |
| NRC | Nuclear Regulatory Commission |
| NRR | Noise Reduction Rating |
| NRRPT | National Registry of Radiation Protection Technologist |
| NSSC | NASA Shared Services Center |
| NVLAP | National Voluntary Laboratory Accreditation Program |
| OCHMO | Office of the Chief Health and Medical Officer |
| OEL | Occupational Exposure Limit |
| OFI | Opportunity for Improvement |
| OH | Occupational Health |
| OHC | Occupational Hearing Conservationist |
| OCHCO | Office of the Chief Human Capital Officer |
| OHP | Occupational Health Program |
| OM | Occupational Medicine |
| OPM | Office of Personnel Management |
| OSHA | Occupational Safety and Health Administration |
| OSMA | Office of Safety and Mission Assurance |
| PA | Posterior to Anterior (Chest x-ray view) |
| PAAMHR | Predicted Age Adjusted Maximum Heart Rate |
| PAP | Papanicolaou Smear |
| PAPR | Powered Air Purifying Respirator |
| PARQ | Physical Activity Readiness Questionnaire |
| PCB | Polychlorinated Biphenyls |
| PEL | Permissible Exposure Limit |
| PII | Personally Identifiable Information |
| PLHCP | Physician or other Licensed Health Care Provider |
| PMD | Private Medical Doctor |
| PNS | Peripheral Nervous System |
| POC | Point of Contact |
| PPD | Purified Protein Derivative used in TB Skin Testing |
| PPE | Personal Protective Equipment |
| PSA | Prostate Specific Antigen |
| QA | Quality Assurance |
| REL | Recommended Exposure Limit |
| RF | Radio Frequency |
| RG | Risk Group |
| RSC | Radiation Safety Committee |
| RSO | Radiation Safety Officer |
| RTW | Return To Work |
| SAARIS | Surveys, Audits, Assessments and Reviews Information System |
| SAE | Society of Automotive Engineers |
| SCAPE | Self-Contained Atmospheric Protective Ensemble |
| SEG | Similar Exposure Groups |
| SEHO | Senior Environmental Health Officer (Agency) |
| SGPT | Alanine Transaminase |
| SOAP | Subjective Objective Assessment Plan |
| SPL | Sound Pressure Level |
| STS | Standard Threshold Shift |
| TAL | Transoceanic Abort Landing |
| TAT | Threat Assessment Team |
| TB | Tuberculosis |
| Td | Tetanus, Diphtheria |
| Tdap | Tetanus, Diphtheria, and Pertussis |
| TDI | Toluene Diphenyl Isocyanate or Toluene Diisocyanate |
| TLV | Threshold Limit Value |
| TSC | Temperature Controlled for Safety |
| TSCA | Toxic Substances Control Act |
| TWA | Time Weighted Average |
| ug | Microgram |
| um | Micrometer |
| USCG | United States Coast Guard |
| USDA | United States Department of Agriculture |
| USPSTF | U.S. Preventive Services Task Force |
| ViTS | Video Teleconferencing Service |
| VOC | Volatile Organic Compound |
| WBC | White Blood Count |
| WC | Workers' Compensation |
| WCO | Workers' Compensation Office |
| WEEL | Workplace Environmental Exposure Levels |
| WHO | World Health Organization |
| ZPP | Zinc Protoporphyrin |
| Exam | Regulation | |
|---|---|---|
| A. | Arsenic | 29 CFR § 1910.1018 |
| B. | Asbestos | 29 CFR § 1910.1001 29 CFR § 1926.1101 |
| C. | Benzene | 29 CFR § 1910.1028 |
| D. | Beryllium | 29 CFR § 1910.1024 |
| E. | Cadmium | 29 CFR § 1910.1027 29 CFR § 1926.1127 |
| F. | Chromium | 29 CFR § 1910.1026 29 CFR § 1926.1126 |
| G. | Ethylene Oxide | 29 CFR § 1910.1047 |
| H. | Formaldehyde | 29 CFR § 1910.1048 |
| I. | Hydrazines | NIOSH Occupational Safety and Health Guideline for Hydrazine, 1988 |
| J. | Isocyanates | NIOSH |
| K. | Lead | 29 CFR § 1910.1025 29 CFR § 1926.62 |
| L. | Mercury | OSHA CPL 02-02-006 NIOSH, ATSDR |
| M. | Methylene Chloride | 29 CFR § 1910.1052 ATSDR |
| N. | 4,4' Methylenebis (2-chloroaniline) (MOCA, MBOCA) | NIOSH, ATSDR, OSHA |
| O. | 4,4' Methylenedianiline (MDA) | 29 CFR §§ 1910.19, 1910.1050 and 1926.60 |
| P. | Nitrogen Tetroxide (Dioxide) | NIOSH Pocket Guide to Chemical Hazards |
| Q. | Polychlorinated Biphenyls (PCB) | ATSDR NIOSH Current Intelligence Bulletin 45, February 24, 1986 NIOSH Pocket Guide to Chemical Hazards |
| R. | Silica Dust | 29 CFR § 1910.1053 |
| S. | Trichloroethylene | NIOSH |
| Exam | Regulation | |
|---|---|---|
| A. | Bloodborne Pathogens | 20 CFR § 1910.1030 |
| B. | Chemistry Laboratory | 29 CFR § 1910.1450 |
| C. | Hazardous Waste Operations and Emergency Response | 29 CFR § 1910.120 |
| D. | Health Care Provider | 29 CFR § 1910.1030, CDC |
| E. | Ionizing Radiation | OSHA 29 CFR §§ 1910.1096, 10 CFR § 20.1502 |
| F. | Lasers | ANSI Z 136.1 |
| G. | Noise | 29 CFR § 1910.95 NPR 1800.1D Chapter 4.8 |
| H. | Pesticides | NIOSH |
| I. | Spray Painting | |
| J. | Water and Sewage | NIOSH |
| K. | Welding | NIOSH Criteria Document No. 88-110 |
| Exam | Regulation | |
|---|---|---|
| A. | Childcare Workers | |
| B. | Confined Space/Tank Entry | 29 CFR § 1910.134 |
| C. | Crane Operator/Ground Floor/Remote-Operation/High/Cabin/Pulpit | NASA STD 8719.9 ASME B30.5-2011 49 CFR subpt. E |
| D. | Diver | 29 CFR § 1910.423 29 CFR § 1910.424 |
| E. | DOT/Commercial Driver License/Motor Vehicle Certification/Multiple Passenger Van | 49 CFR subpt. E |
| F. | Down Range/Shipboard Duty | 46 CFR subpts. 10 and 12 |
| G. | Firefighter | NFPA 1582 |
| H. | Food Handler | 46 CFR § 12.25-20 NPR 1800.1 Chapter 4.10 |
| I. | Locomotive Engineer | 49 CFR § 240.121 |
| J. | Motive (Heavy) Equipment Operator | 49 CFR subpt. E |
| K. | Occupational Respirator Use | 29 CFR § 1910.134 29 CFR § 1910.134 Appendix A |
| L. | Ordnance Handler | NAVMED P-117, 15-107, AFI132-3001 |
| M. | Primary Animal Contact | |
| N. | Primary Crew Contact | JSC 22538 |
| O. | Security | |
| P. | Self-Contained Atmospheric Protective Ensemble | 29 CFR § 1910.134 |
| Q. | Soldering | IPC J-STD-001ES |
| R. | Voluntary Respirator Use | 29 CFR § 1910.134 29 CFR § 1910.134 Appendix A |
| Exam | Regulation | |
|---|---|---|
| A. | NASA Pilots, Flight Engineers, Other Primary Aircrew, Qualified Non-Crewmember, Unmanned Aircraft System (UAS) Pilots and Observers | OCHMO 110902MED, NPR 7900.3, 14 CFR pt. 67 |
| B. | Air Traffic Control Specialist (Not Requiring FAA Certification) | OPM GS-2152 |
| C. | Second Class Airman's Medical Certification (Air Traffic Control Tower Operator) | 14 CFR pt. 67 Appendix A |
| Exam | Regulation | |
|---|---|---|
| A. | Fitness for Duty | NPR 1800.1 |
| B. | Return to Work | NPD 1840.1 NPR 1800.1 |
| C. | International Travel | NPR 1810.1 |
| Exam | Regulation | |
|---|---|---|
| A. | Preventive Health Examination | USPSTF |
| B. | Fitness Center Clearance | NPR 1800.1 |
| A. Arsenic | |
|---|---|
| Reference | OSHA 29 CFR § 1910.1018 |
| Frequency |
1. Baseline Examination 2. Annual Exam, if less than 45 years old 3. Semiannually, if 45 years old or older, or with 10 or more years of exposure 4. Variable or Exposure-Determined Examination 5. Exit/Reassignment Examination |
| Laboratory |
1. Chest X-ray (PA), annual 2. Discretionary Tests a. Pulmonary Function b. Complete Blood Count |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on peripheral and CNS, GI system, skin including nasal mucosa, respiratory tract, and thyroid 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Liver, kidneys, skin, lungs, lymphatic system, CNS, PNS |
| Written Opinion | Standard Written Medical Opinion |
| Employee Counseling | Counseling on exam results and conditions of increased risk |
| Medical Removal | No requirement in standard |
| B. Asbestos | |
|---|---|
| Reference |
OSHA 29 CFR § 1910.1001 OSHA 29 CFR § 1926.1101 |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Variable or Exposure-Determined Examination 4. Exit/Reassignment Examination |
| Laboratory (TX) 1. |
1. Chest X-ray (PA) (Must be read by "B reader", a board eligible/certified radiologist, or an experienced physician with known expertise in pneumoconiosis.):
a. Baseline
2. Pulmonary Function b. Periodic: i. 1-10 years since first exposure: 1. every 5 years ii. 10+ years since first exposure, and:
1. below age 35, every 5 years
2. age 35-45, every 2 years 3. age 45+, annually 3. Discretionary Tests
a. Hemoccult
b. Annual TB Screening c. Urinalysis (dipstick) |
| Physical Exam |
1. Required Asbestos Questionnaire (Standardized on initial exam, Abbreviated Standardized on annual exam) 2. Physical Examination with focus on respiratory, CV, and GI systems 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Respiratory/lungs, pleural (Mesothelioma), gastrointestinal |
| Written Opinion | Standard Written Medical Opinion for Asbestos within 30 days, including statement that employee was informed of the increased risk of lung cancer attributable to combined effect of smoking and asbestos. |
| Employee Counseling | Exam results and conditions of increased risk including increased risk of lung cancer from combined effects of smoking and asbestos exposure |
| Medical Removal | No requirement in standard |
| C. Benzene | |
|---|---|
| Reference | OSHA 29 CFR § 1910.1028 |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Variable or Exposure-Determined Examination |
| Laboratory |
1. Complete Blood Count (CBC) including a leukocyte count with differential, a quantitative thrombocyte count, hematocrit, hemoglobin, erythrocyte count, and erythrocyte indices (MCV, MCH, MCHC). (Repeat within 2 weeks if abnormal, refer to standard for action level) 2. Pulmonary Function (if employee wears respirator, initial exam and then every 3 years) 3. For Emergency Exposures Only:
a. Urine sample provided at the end of employee's shift for urinary phenol test within 72 hours and urine specific gravity corrected to 1.024.
4. Discretionary Tests:b. If urinary phenol test is equal to or greater than 75 mg phenol/L of urine, repeat Complete Blood Count monthly for 3 months.
a. Refer to Appendix C of standard for guidance
|
| Physical Exam |
1. Detailed Medical and Occupational History initially, brief update annually 2. Complete Physical Examination with focus on the blood, skin, CNS, and liver and kidney function 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Eyes, respiratory, CNS, skin, blood/bone marrow |
| Written Opinion | Standard Written Medical Opinion within 15 days |
| Employee Counseling | Counseling on exam results and conditions of increased risk |
| Medical Removal | Required when referred to hematologist/internist |
| D. Beryllium | |
|---|---|
| Reference | 29 CFR § 1910.1024 |
| Frequency | 1. Baseline Examination |
| Laboratory | 1. Be-LPT or equivalent |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on skin, eyes, and respiratory tract 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Respiratory, skin |
| Written Opinion | Written opinion to employee within 45 days to include explanation of examination results and detection of medical conditions such as chronic beryllium disease (CBD), beryllium sensitization and medical conditions related to airborne exposures that require further evaluation.
Written opinion to the employer within 45 days that examination has met the requirement of the standards,recommendations on limitations for use of protective equipment, including respirators, and that results have been explained to the employee. If employee gives written authorization opinion may include recommendation for medical removal due to confirmed CBD or referral to CBD diagnostic center. |
| Employee Counseling | Counseling on exam results and conditions, risks related to beryllium exposure that requires further evaluation, treatment or lifestyle modification. |
| Medical Removal | Required based upon medical recommendation |
| Multiple Physician Review Process | Referral to CBD if recommended by provider. |
| E. Cadmium | |
|---|---|
| Reference |
OSHA 29 CFR § 1910.1027 OSHA 29 CFR § 1926.1127 |
| Frequency |
1. Baseline Examination 2. Annual Examination 1 year following Baseline Examination 3. Biennially Examination (see standard for guidance on frequency with abnormal laboratory findings) 4. Variable or Exposure-Determined Examination 5. Exit/Reassignment Examination |
| Laboratory |
Annual Laboratory: 1. Cadmium in urine (CdU) (See Appendix F for protocol for sample handling and laboratory selection) 2. Beta-2 microglobulin in urine (B(2)-M) 3. Cadmium in blood (CdB) 4. BUN and Serum Creatinine 5. Complete Blood Count (CBC) 6. Chest X-ray (PA)
a. Baseline
7. Pulmonary Functionb. Exit/Reassignment 8. Discretionary Tests:
a. Annual Chest X-ray
b. PSA (for males 50 years and older) c. Urinalysis |
| Physical Exam |
1. Cadmium Exposure Questionnaire required (Appendix D in CFR) 2. Complete Physical Examination with focus on blood pressure, respiratory, and urinary systems (refer to health effects Appendix A) 3. Prostate palpation, males 40 years and older 4. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Written Opinion | Standard Written Medical Opinion for Cadmium |
| Employee Counseling | Counseling on exam results and medical conditions related to cadmium exposure requiring further evaluation or treatment or removal. |
| Medical Removal | Required |
| Multiple Physician Review Process | Required if requested by examinee (see CFR) |
| F. Chromium | |
|---|---|
| Reference | OSHA 29 CFR §1910.1026, 29 CFR § 1926.1126 |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Variable or Exposure-Determined Examination 4. Exit/Reassignment Examination |
| Laboratory | Discretionary |
| Physical Exam |
1. Medical and Occupational History 2. Physical Exam with focus on skin and respiratory tract |
| Target Organs | Respiratory, liver, kidney, eye, skin |
| Written Opinion | Standard Written Medical Opinion within 30 days | Employee Counseling | Counseling on exam results and conditions of increased risk |
| Medical Removal | No requirement in standard |
| G. Ethylene Oxide | |
|---|---|
| Reference | OSHA 29 CFR § 1910.1047 |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Variable or Exposure-Determined Examination 4. Exit/Reassignment Examination |
| Laboratory |
1. Complete Blood Count (CBC) with differential 2. Discretionary Tests:
a. Pregnancy test, if requested by employee
b. Laboratory evaluation of fertility if requested by examinee and considered appropriate by provider c. Blood Chemistry Panel d. Urinalysis |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on pulmonary, hematologic, neurologic, and reproductive system, and eyes and skin. 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Respiratory, blood, CNS, reproductive, eye, skin, liver, kidney |
| Written Opinion | Standard Written Medical Opinion within 15 days |
| Employee Counseling | Counseling on exam results and conditions of increased risk |
| Medical Removal | No requirement in standard |
| H. Formaldehyde | |
|---|---|
| Reference | OSHA 29 CFR § 1910.1048 |
| Frequency |
1. Baseline Examination 2. Annual Examination (for employees required to wear respirator, others discretionary) 3. Variable or Exposure-Determined Examination 4. Exit/Reassignment Examination |
| Laboratory |
1. Pulmonary Function (for required respirator use)
a. Baseline
b. Annual |
| Physical Exam | 1. Medical and Occupational History (nonmandatory medical disease questionnaire
- Appendix D in CFR is recommended) 2. Physical Examination with focus on eyes, skin, mucous membranes, and allergies and allergic reactions 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Respiratory, eyes, skin |
| Written Opinion | Standard Written Medical Opinion for Formaldehyde within 15 days of results |
| Employee Counseling | Counseling on exam results and conditions of increased risk including whether medical conditions were caused by past or emergency exposures. |
| Medical Removal | Required |
| Multiple Physician Review Process | Required if requested by examinee (see CFR) |
| I. Hydrazines | |
|---|---|
| Reference | NIOSH Occupational Safety and Health Guideline for Hydrazine, 1988 |
| Frequency |
1. Baseline Examination 2. Annual Examination |
| Laboratory |
1. Baseline Chest X-ray 2. Complete Blood Count 3. Liver Profile 4. Urinalysis with microscopic 5. Discretionary:
a. Pulmonary Function
|
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Eyes, respiratory, skin, CNS, liver, kidneys |
| Written Opinion | No requirement in standard |
| Employee counseling | Counseling on exam results and conditions of increased risk |
| Medical Removal | No requirement in standard |
(e.g., Methylene Diisocyanate (MDI), Toluene Diisocyanate (TDI).)
|
|
|---|---|
| Reference | NIOSH 78-215 |
| Frequency |
1. Baseline Examination 2. Variable or Exposure Determined Examination 3. Annual Examination |
| Laboratory |
1. Pulmonary Function 2. Chest X-ray (PA) at 5-year intervals |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on respiratory system, skin, and mucous membranes (Isocyanates are potent sensitizers. Acute exposures may cause severe airway obstruction.) 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Eyes, respiratory, kidney, liver, skin, CNS |
| Written Opinion | No requirement in standard |
| Employee Counseling | Counseling on exam results and conditions of increased risk and delayed effects such as coughing or difficulty breathing at night. |
| Medical Removal | No requirement in standard |
| K. Lead | |
|---|---|
| Reference |
OSHA 29 CFR § 1910.1025 OSHA 29 CFR § 1926.62 |
| Frequency |
1. Baseline Examination 2. Annual Examination for employee's with blood lead over 40ug/100g in the preceding 12 months 3. Variable or Exposure-Determined Examination 4. Exit/Reassignment Examination |
Laboratory |
1. Blood Lead and ZPP (Baseline and every 6 months) 2. If Blood Lead is at or above 40ug/100g, repeat every 2 months 3. Repeat blood lead 2 weeks after any test is at or above 60ug/100g (requires medical removal) 4. During Medical Removal, Blood Lead and ZPP monthly 5. Hemoglobin and Hematocrit, red cell indices, and examination of peripheral smear morphology 6. BUN and Serum Creatinine 7. Urinalysis with microscopic 8. Discretionary Tests:
a. Pregnancy/fertility testing, if employee requests
|
| Physical Exam |
1. Medical and Occupational History 2. Complete Physical Examination with focus on teeth, gums, hematological, GI, CV, renal, and neurological system. 3. Blood Pressure 4. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Pulmonary, kidney, blood, reproductive, CNS, gastrointestinal, CV, gums, teeth, eyes |
| Written Opinion | Standard Written Medical Opinion for all evaluations and employee written notification of blood level results over 40ug/100g within 5 business days | Employee Counseling | Counseling on exam results and conditions of increased risk including advising of occupational and non-occupational conditions requiring further examination or treatment. |
| Medical Removal | Required (see CFR for criteria) |
| Multiple Physician Review Process | Required if requested by examinee (see CFR) |
| L. Inorganic Mercury | |
|---|---|
| Reference | OSHA CPL 02-02-06 |
| Frequency |
1. Baseline Examination 2. Annual Interim History 3. Variable or Exposure-Determined Examination |
| Laboratory |
1. Complete Blood Count (CBC) 2. Urinalysis 3. Voluntary pregnancy test, where appropriate 4. Urine mercury level (for history of exposure, recommend all employees in given work area be tested at the same time). If exposed above PEL test every 3 months, if below PEL test every 6 months. |
| Physical Exam |
1. Medical and Occupational History (annual interim history) 2. Physical Examination with focus on central nervous and respiratory systems, kidneys, and skin. 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Liver, kidney, CNS, PNS, lung, eye, mucous membranes |
| Written Opinion | Standard Written Medical Opinion |
| Employee Counseling | Counseling on exam results and conditions of increased risk and any medical conditions which require further examination or treatment. |
| Medical Removal | No requirement in standard |
| M. Methylene Chloride | |
|---|---|
| Reference | OSHA 29 CFR § 1910.1052 |
| Frequency |
1. Baseline Examination 2. Annual Medical and Occupational History Update 3. Examination Frequency Age Determined: a. Annual, if age 45 or older b. Every 36 months under age 45 4. Variable or Exposure-Determined Examination 5. Exit/Reassignment Examination |
| Laboratory |
1. Discretionary:
a. Pulmonary Function
b. Hemoglobin and Hematocrit c. ALT, SGPT d. Post-shift Carboxyhemoglobin e. ECG |
| Physical Exam |
1. Methylene Chloride Questionnaire required (annual interim history-CFR Appendix B) 2. Physical Examination focus on employee health status and analysis of questionnaire responses 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Respiratory, CV, liver, CNS, skin, blood |
| Written Opinion |
Standard Written Medical Opinion for Methylene Chloride with the following within 15 days of completion of medical and laboratory findings but not more than 30 days past examination including:
a. Statement that the physician has informed the employee Methylene Chloride (MC) is a potential carcinogen risk
b. The risk factors for heart disease, and the potential exacerbation of underlying heart disease from MC exposure and its metabolism to carbon monoxide |
| Employee Counseling | Counseling on exam results and that MC is a potential occupational carcinogen, risk factors for heart disease and potential exacerbation of underlying heard disease by exposure to MC through metabolism of carbon monoxide. |
| Medical Removal | Required |
| Multiple Physician Review Process | Required if requested by examinee (see CFR) |
| N. 4,4' Methylenebis (2-chloroaniline) (MOCA, MBOCA) | |
|---|---|
| Reference | NIOSH Publication No. 78-188 |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Laboratory only every 6 months (employees working directly in production or handling for 10 years or longer) |
| Laboratory |
1. Complete Blood Count (CBC) 2. Blood Chemistry Profile (to include LFTs) 3. Urinalysis with microscopic 4. Chest X-ray (discretionary) |
| Physical Exam |
1. Medical and Occupational History 2. Focused Physical Examination |
| Target Organs | Liver, blood, kidneys |
| Written Opinion | No requirement in standard |
| Employee Counseling | Counseling on exam results and conditions of increased risk |
| Medical Removal | No requirement in standard |
| O. 4,4' Methylenenedianiline (MDA) | |
|---|---|
| Reference | OSHA 29 CFR § 1910.1050 |
| Frequency |
1. Baseline Examination 2. Annual Examination |
| Laboratory |
1. Blood Chemistry Profile (to include LFTs) 2. Urinalysis with microscopic |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on skin disease and liver dysfunction 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Skin, eyes, liver, CV, spleen | Written Opinion | Standard Written Medical Opinion required |
| Employee Counseling | Counseling on exam results and conditions of increased risk |
| Medical Removal | Required |
| Multiple Physician Review Process | Required if requested by examinee (see CFR) |
| P. Nitrogen Tetroxide (Dioxide) | |
|---|---|
| Reference | NIOSH Pocket Guide to Chemical Hazards-Nitrogen Dioxide |
| Frequency | Baseline Examination |
| Laboratory |
1. Discretionary
a. CBC with diff
b. PFT c. EKG d. CXR |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on pulmonary system, skin, and eyes |
| Target Organs | Eyes, respiratory, CV |
| Written Opinion | No requirement in standard |
| Employee Counseling | Counseling on exam results and conditions of increased risk |
| Medical Removal | No requirement in standard |
| Q. Polychlorinated Biphenyls (PCB) | |
|---|---|
| Reference | NIOSH Current Intelligence Bulletin 45, February 24, 1986, NIOSH Pocket Guide to Chemical Hazards-Polychlorinated Biphenyls |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Variable or Exposure-Determined Examination 4. Exit/Reassignment Examination |
| Laboratory |
1. Blood Chemistry 2. Complete Blood Count 3. Urinalysis 4. Chest x-ray (baseline) 5. Discretionary Tests:
a. ECG
b. Pulmonary Function c. Fecal Occult |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on the skin, liver, and nervous system. 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Skin, eyes, liver, reproductive system |
| Written Opinion | No requirement in standard |
| Employee Counseling | Counseling on exam results and conditions of increased risk |
| Medical Removal | No requirement in standard |
| R. Silica Dusts | |
|---|---|
| Reference | 29 CFR § 1910.1053 |
| Frequency | 1. Baseline Examination |
| Laboratory | 1. Chest X-ray (Must be read by NIOSH-certified B Reader) |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on respiratory system 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Lungs/respiratory |
| Written Opinion | Written opinion to employee within 30 days including: the results of the examination, conditions that place employee at increased risk due to exposure to silica, conditions that require further evaluation, recommended limitations on respirator use, limitations on exposure to silica and recommendations for referral to a specialist. Written opinion to employer including statement that examination met the requirements of the standard, recommended limitations of respirator use. If employee gives written authorization opinion may include recommended limitations to exposure to silica and recommended referral to a specialist. |
| Employee Counseling | Counseling on exam results and conditions of increased risk and any medical conditions which require further examination or treatment. |
| Medical Removal | No requirement in standard |
| S. Trichloroethylene | |
|---|---|
| Reference | NIOSH Pocket Guide to Chemical Hazards-Trichloroethylene |
| Frequency |
1. Baseline Examination 2. Annual Examination |
| Laboratory |
Discretionary
a. LFTs
b. PFTs c. Urinalysis d. Blood Chemistry e. Complete Blood Count f. Visual acuity |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on cardiac, pulmonary, liver, and kidneys 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Respiratory, CV, kidney, liver, skin, CNS, eyes |
| Written Opinion | No requirement in standard |
| Employee Counseling | Counseling on exam results and conditions of increased risk |
| Medical Removal | No requirement in standard |
| A. Bloodborne Pathogens | |
|---|---|
| Reference | OSHA 20 CFR § 1910.1030 |
| Frequency |
1. Baseline Examination (for occupational groups covered under the standard) 2. Variable or Exposure-Determined Examination |
| Laboratory |
1. Hepatitis B Vaccine 2. Hepatitis B Surface antibody (HepBSAb)Titer (required one time only after 3rd dose completed) 3. Declination statement must be signed if Hepatitis B Vaccine declined by employee (Appendix A of OSHA Standard) 4. Discretionary: Post-exposure
a. Victim: HIV test, HepBSAb if not already documented, and HepCAb (other tests per provider)
b. Source (after consent given): HIV test (rapid screen if available), HepB Surface Antigen (HepBSAg), and HepCAb (other tests per provider) c. If any HIV test is performed because of a specific occupational exposure, then a confidential ID system and a secure method to receive the test results shall be insured for both victim and source. |
| Physical Exam |
1. Medical and Occupational History 2. Focused Physical Examination (discretionary) |
| Target Organs | Multiple organs |
| Written Opinion | Standard Written Medical Opinion required within 15 days of completion of evaluation including whether Hepatitis B immunization is indicated and if the employee has received such vaccine |
| Employee Counseling |
Counseling on exam results and conditions of increased risk. Post exposure counseling regarding HBV vaccine and follow-up. |
| Medical Removal | No requirement in standard |
| B. Chemical Laboratory | |
|---|---|
| Reference | OSHA 29 CFR § 1910.1450 |
| Frequency | Variable or Exposure-Determined Examination |
| Laboratory |
1. Discretionary:
a. Blood Chemistry Profile
b. Complete Blood Count (CBC) c. Chest X-ray d. Pulmonary Function e. Urinalysis f. Visual Acuity |
| Physical Exam |
1. Medical and Occupational History 2. Focused Physical Examination 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Multiple organs, especially eyes, skin, liver |
| Written Opinion | Standard Written Opinion required |
| Employee Counseling | Counseling on exam results and conditions of increased risk |
| Medical Removal | No requirement in standard |
| C. Hazardous Waste Operations and Emergency Response | |
|---|---|
| Reference | OSHA 29 CFR § 1910.120, Occupational Safety and Health Guidance Manual for Hazardous Waste Site Activities |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Variable or Exposure-Determined Examination 4. Exit/Reassignment Examination |
| Laboratory |
1. Audiogram (Baseline) 2. Visual Acuity, Color Discrimination, Visual Fields 3. Complete Blood Count (CBC) 4. Blood Chemistry 5. Urinalysis 6. Chest X-Ray (Baseline) 7. Discretionary Tests:
a. ECG
b. Exercise Stress Test c. Pulmonary Function d. Other based on specific exposure (see Guidance Manual) e. Chest X-Ray (Follow-up) |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on worker's fitness, including ability to wear any required PPE, back or musculoskeletal problems, heat stress, claustrophobia 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use 4. Employee may also be covered by Bloodborne Pathogen standard |
| Target Organs | Multiple organs |
| Written Opinion |
Standard Written Medical Opinion required including:
a. Statement that the employee has sufficient strength, endurance, and emotional stability to perform the work
b. Opinion that no medical condition was detected which would place the employee at increased risk of material impairment of the employee's health or would be a hazard to self or others from hazardous waste operations, emergency response, or respirator use c. Any limitations in job functions or ability to wear PPE d. The results of the medical examination and tests were also provided if requested by the employee |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| Medical Removal | No requirement in standard |
| NOTE regarding eligibility |
Protocol covers the following employees:
a. Potentially exposed to hazardous substances, without regard to the use of respirator, for more than 30 days per year
Employees Not Covered in Standard:b. Required to use a respirator more than 30 days per year c. Injured from exposure of hazardous substances during an emergency incident d. Members of a HazMat team
a. Emergency responders not designated members of HazMat team (e.g., security, firefighters)
|
| D. Healthcare Provider | |
|---|---|
| Reference | OSHA 20 CFR § 1910.1030 |
| Frequency |
1. Baseline Examination 2. Variable or Exposure-Determined Examination |
| Laboratory |
1. Hepatitis B Vaccine (required or declination letter shall be completed) or demonstrated immunity 2. TB Screening required for baseline, periodic testing is discretionary based on risk assessment for the facility 3. Discretionary:
a. Hepatitis Profile
b. Measles, Mumps, Rubella Vaccine c. Diphtheria, Tetanus, and Pertussis (Td, Tdap) d. Varicella Vaccine (if no history of chicken pox) e. Influenza Vaccine offered annually |
| Physical Exam |
1. Medical and Occupational History 2. Focused Physical Examination (discretionary) 3. Employee also covered by Bloodborne Pathogen Standard |
| Target Organs | Respiratory, blood, liver, skin |
| Written Opinion | No requirement in standard |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| Medical Removal | No requirement in standard |
| E. Ionizing Radiation | |
|---|---|
| Reference | OSHA 29 CFR § 1910.1096, 10 CFR § 20.1502 |
| Frequency | Variable or Exposure-Determined Examination |
| Laboratory | Complete Blood Count (CBC) with Differential |
| Physical Exam |
1. Medical and Occupational History including exposure 2. Focused Physical Examination |
| Target Organs | Exposure determined |
| Written Opinion | No requirement in standard |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| Medical Removal | No requirement in standard |
| F. Lasers | |
|---|---|
| Reference |
ANSI Z 136.1 (2014), Required for Class 3B and Class 4 Lasers NOTE: Baseline examinations are not mandatory but encouraged to serve as a basis for comparison in the event of a mishap. Centers should establish a uniform policy applicable to all employees working with Class 3B and 4 lasers. |
| Frequency |
1. Baseline Examination (per Center Policy) 2. Variable or Exposure-Determined Examination (within 48 hours) |
| Laboratory |
1. Visual Acuity with refraction corrections to 20/20 (6/6) far and near vision (more extensive examination indicated if this is not met - see standard) 2. Amsler Grid (or similar pattern to test macular function for vision distortions and scotomas) 3. Color Vision Discrimination (Ishihara or similar color vision test) 4. Ocular fundus Examination with Ophthalmoscope or appropriate Fundus Lens at a Slit Lamp if visual acuity, macular function, or color vision is abnormal. Dilated exam required if abnormalities found. |
| Physical Exam |
1. Medical, Occupational, and Ocular History 2. Focused Physical Examination performed by or under supervision of ophthalmologist, optometrist, or other qualified physician 3. Limited skin examination |
| Target Organs | Eye, skin |
| Written Opinion | No requirement in standard |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| Medical Removal | No requirement in standard |
| G. Noise | |
|---|---|
| Reference | OSHA 29 CFR § 1910.95, NPR 1800.1 Chapter 4.8 |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Exit/Reassignment Examination |
| Laboratory |
1. Baseline Audiogram or within 30 days 2. Audiogram Annually 3. Retest (audiogram) within 30 days if there is a STS |
| Physical Exam |
1. Medical and Occupational History 2. Focused Physical Examination with focus on external and tympanic membrane |
| Target Organs | Ears and hearing system |
| Written Opinions | Required within 21 days of Standard Threshold Shift (STS) determination including statement that STS has occurred, whether further evaluation and testing indicated, and opinion on work relatedness or aggravation by occupational noise exposure, and limitation in use of protective hearing equipment |
| Employee Counseling | Counseling if STS or suspected ear pathology |
| Medical Removal | No requirement in standard |
| H. Pesticide | |
|---|---|
| Reference | NIOSH Pocket Guide the Chemical Hazards |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Variable or Exposure-Determined Examination 4. Exit/Reassignment Examination |
| Laboratory |
1. Baseline (required before occupational exposure)
Plasma and RBC cholinesterase baselines should be established by performing each test twice (3 to 7 days between tests) and averaging the result for the baseline for each.
2. Blood Chemistry 3. Urinalysis (dipstick) 4. Discretionary Tests:
a. Pulmonary Function
b. RBC cholinesterase levels for recent exposure c. Plasma cholinesterase for acute exposure |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on the skin and nervous system 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Target Organs | Kidney, liver, CNS, skin, lung |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| Medical Removal | If plasma or RBC cholinesterase activity is decreased by 30 percent or greater from baseline the employee should be removed from exposure until follow-up test levels are at least 80 percent of baseline. |
| I. Spray Painting | |
|---|---|
| Reference | |
| Frequency |
1. Baseline Examination 2. Variable or Exposure-Determined Examination |
| Laboratory |
Discretionary Tests:
a. Blood Chemistry Profile
b. CBC c. Chest X-ray d. Urinalysis e. Pulmonary Function Test |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination (discretionary) 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use 4. Evaluation of other potential exposures, e.g. lead |
| Target Organs | Exposure determined |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| Medical Removal | Exposure determined, e.g. lead |
| J. Water and Sewage | |
|---|---|
| Reference | NIOSH Publication 2002-149 |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Variable or Exposure-Determined Examination |
| Laboratory |
1. Immunizations offered:
a. Tetanus Diphtheria (Td) Vaccine
2. Discretionary Tests:b. Hepatitis A and B Vaccine
a. Blood Chemistry Profile b. Complete Blood Count (CBC) c. Chest X-ray |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination (discretionary) |
| Target Organs | Liver, gastrointestinal, blood |
| Written Opinion | No requirement |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| Medical Removal | No requirement |
| K. Welding | |
|---|---|
| Reference | NIOSH Criteria Document No. 88-110 |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Variable or Exposure-Determined Examination |
| Laboratory |
1. Pulmonary Function (Base only) 2. Blood Chemistry Profile 3. Complete Blood Count (CBC) 4. Urinalysis 5. Visual Acuity, Depth Perception, and Color Discrimination 6. Chest X-ray (Baseline)
Skin exam (burns, chronic damage)
|
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on skin, respiratory, macular, cornea, fundus, and any condition that may interfere with ability to perform duties 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination Occupational Respirator Use 4. Evaluation of other potential exposures, e.g. metals, flux, compounds |
| Target Organs | Respiratory, eyes, varies with exposure type |
| Written Opinion | No requirement in standard |
| Employee Counseling | Counseling on exam results and conditions of increased risk, including smoking. |
| Medical Removal | Exposure determined, e.g. lead |
| A. Childcare Workers | |
|---|---|
| Reference | |
| Frequency |
1. Baseline Examination 2. Variable or Exposure-Determined Examination |
| Laboratory |
1. Annual TB Screening 2. Discretionary Vaccines offered:
a. Influenza
b. Measles, Mumps, and Rubella (MMR) c. Tetanus/Diphtheria (Td) d. Polio e. Hepatitis A f. Chickenpox g. Hepatitis B |
| Physical Exam |
1. Medical and Occupational/Immunization History 2. Physical Exam with focus on ability to lift and bend repetitively |
| Target Organs | Musculoskeletal |
| Written Opinion | Job Certification with any limitations | .
| Employee Counseling | Counseling on exam results and conditions of increased risk | .
| B. Permit-Entry Confined Space/Tank Entry | |
|---|---|
| Reference | 29 CFR § 1910.134 |
| Frequency | 1. Variable or Exposure-Determined Examination |
| Laboratory |
1. Audiogram 2. Visual Acuity, Depth Perception, and Color Vision (or demonstration of employee's ability to see and hear warnings, such as flashing lights, buzzers, and sirens) 3. Discretionary Tests:
a. ECG
b. Chest X-ray (Baseline) c. Urinalysis (dipstick) d. Pulmonary Function |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on employee's ability to carry out assigned duties and detection of any disease or abnormality that would make it difficult to work within confined spaces 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use 4. Evaluation of other exposures may be required |
| Written Opinion | Job Certification with any limitations |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
|
C. Crane Operators/Riggers NOTE: Includes ground floor, remote operation, high, cabin, pulpit |
|
|---|---|
| Reference |
National Commission for the Certification of Crane Operators NASA STD 8719.9 49 CFR subpt. E |
| Frequency |
1. Baseline Examination 2. Every 3 years |
| Laboratory |
1. Audiogram: Hearing threshold average in better ear < 40 dB (500, 1000, 2000 Hz) 2. Visual Acuity: Minimum of 20/40 Snellen in each eye without correction or separately corrected to 20/40 Snellen in both eyes with or without corrective lenses 3. Depth Perception 4. Field of vision at least 70 degrees in the horizontal median in each eye 5. Color Vision 6. Discretionary Tests:
a. ECG
b. Urinalysis c. Pulmonary function d. Hemoglobin (Hgb) and Hematocrit (Hct ) e. HbA1C (discretionary) |
| Physical Exam |
Complete examination: 1. History to ascertain any condition that may cause any sudden incapacitation or inability to perform duties 2. Evaluation for reaction time, manual dexterity, and coordination 3. No tendencies to seizures, dizziness, claustrophobia, sudden incapacitation, loss of physical control, or similar undesirable conditions such as insulin controlled diabetes 4. No evidence of physical defects, or emotional instability, that in the opinion of the examiner, would present a hazard to self or others |
| Written Opinion | Job Certification with any limitations or referral for additional specialized clinical evaluation or testing
If an employee has Insulin Treated Diabetes Mellitus (ITDM) a Federal Motor Carrier Safety Administration (FMCSA)-compliant waiver is required to obtain a 12-month certification. Each Center with drivers requiring Department of Transportation (DOT) certification will have a Certified Medical Examiner. The Center's Certified Medical Examiner, civil service or contractor (per the contractor's contract) will review 1. The FMCSA ITDM Assessment Form MCSA-5870 from the employee's treating physician, per 49 CFR pt. 46. 2. A letter from employee's supervisor stating. a. The workplace is able to meet requirements to accommodate the employee such as mitigating hypoglycemic symptoms, monitoring glucose levels, and training the employee to recognize hypoglycemic episodes. b. If the crane has a dead-man switch. OCHMO will issue certifications for Centers without a Certified Medical Examiner. Occupational health clinic physicians at Centers without a Certified Medical Examiner will submit the information requested in paragraphs 1 and 2 above, along with a waiver recommendation to OCHMO within 30 days of receipt of the required FMCSA ITDM Assessment Form. |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| D. Diver | |
|---|---|
| Reference | 29 CFR §§ 1910.401-441, subpt. T |
| Frequency |
1. Baseline Examination 2. Annual Exam |
| Laboratory |
1. Audiogram 2. Baseline and Annual ECG 3. Baseline Chest X-ray (PA and lateral) 4. Pulmonary Function (Vital Capacity) 5. Urinalysis (dipstick) 6. Blood Chemistry 7. Complete Blood Count (CBC) 8. TB Screening 9. Visual Acuity and Color Discrimination 10. Discretionary Tests:
a. Exercise Stress Test
|
| Physical Exam |
1. Medical and Occupational History to include predisposition to unconsciousness, vomiting, cardiac arrest, impairment of oxygen transport, serious blood loss, or anything that interferes with effective underwater work 2. Physical Examination |
| Written Opinion | Job Certification with any limitations, or recommend further specialized clinical evaluation or testing |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
|
E. DOT/Commercial Driver License/ Motor Vehicle Certification/Multiple Passenger Van |
|
|---|---|
| Reference | 49 CFR subpt. E |
| Frequency |
1. Baseline Examination 2. Biennial Exam unless more frequent examination is required by the examining provider (per DOT regulations) |
| Laboratory |
1. Forced whisper voice in better ear at not less than 5 feet with or without hearing aid or Audiogram: Hearing threshold average loss in better ear not > 40 dB at 500, 1,000, 2,000 Hz with or without hearing aid 2. Visual Acuity: At least 20/40 (Snellen) in each eye without corrective lenses or visual acuity separately corrected to 20/40 or better with corrective lenses, distant binocular acuity of at least 20/40 in both eyes with or without corrective lenses 3. Depth perception 4. Gross field of vision: 70 degrees in each eye 5. Traffic signal color perception 6. Urinalysis (dipstick) 7. Discretionary Tests:
a. Chest X-ray
b. Complete Blood Count (CBC) c. Blood Chemistry Profile d. ECG e. Exercise Stress Test f. Pulmonary Function |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on any condition that may cause any sudden incapacitation or inability to perform duties, tendencies to seizures, dizziness, claustrophobia, loss of physical control, or similar undesirable conditions (Cannot qualify if diabetic on insulin or if currently on medication for seizure disorder/epilepsy) |
| Written Opinion |
Job Certification with any limitations or referral for additional specialized clinical evaluation or testing
If an employee has Insulin Treated Diabetes Mellitus (ITDM) a FMCSA-compliant waiver is required to obtain a 12-month certification. Each Center with drivers requiring Department of Transportation (DOT) certification will have a Certified Medical Examiner. The Center's Certified Medical Examiner, civil service or contractor (per the contractor's contract) will review 1. The FMCSA ITDM Assessment Form MCSA-5870 from the employee's treating physician, per 49 CFR pt. 46. 2. A letter from employee's supervisor stating the workplace is able to meet requirements to accommodate the employee such as mitigating hypoglycemic symptoms, monitoring glucose levels, and training the employee to recognize hypoglycemic episodes. OCHMO will issue certifications for Centers without a Certified Medical Examiner. Occupational health clinic physicians at Centers without a Certified Medical Examiner will submit the information requested in paragraphs 1 and 2 above, along with a waiver recommendation to OCHMO within 30 days of receipt of the required FMCSA ITDM Assessment Form. |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| F. Down Range/Shipboard Duty | |
|---|---|
| Reference | 46 CFR subpts. 10.205; 12.02-27; 12.25 |
| Frequency |
1. Baseline Examination (temporary assignment to ships, submarines, or NASA Test Range shipboard) 2. Annual Examination (for Masters, Chief Mates, Chief Engineers, 1st Assistant Engineer, Food Handlers, or anyone 60 years and up, or temporary assignments) 3. Variable (if none of the above):
a. Every 5 years for 17 to 24 years of age
b. Every 3 years for 25-49 years of age c. Every 2 years for 50 to 59 years of age |
| Laboratory |
1. Audiogram 2. Visual Acuity: 20/200 correctable to 20/40 (Snellen) for deck responsibility; correctable to 20/50 for engineering responsibility 3. TB Screening 4. Gross Visual Fields: If otherwise qualified, may have lost vision in one eye if remaining good eye's vision is passing 5. Color Perception (Pseudoisochromatic Plates or Eldridge--Green Color Perception Lantern) 6. Discretionary Tests:
a. Chest X-ray
b. ECG c. Travel Immunizations (offered) |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination 3. Shipboard food handlers must abide by the Food Handler protocol |
| Written Opinion | Job Certification with limitations |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| G. Fire Fighter | |
|---|---|
| Reference | National Fire Protection Association (NFPA) 1582 |
| Frequency |
1. Baseline Examination 2. Annual Examination, if 40 or older 3. Biennial Examination, if between ages 30-39 4. Triennial Examination, if 29 or younger |
| Laboratory |
1. Audiogram: Average hearing loss in the unaided better ear less than 40 dB at 500, 1000, 2000, and 3000 Hz. 2. Comprehensive Metabolic Panel (including cholesterol, HDL, LDL, triglycerides, lipid ratios, LFTs) 3. CBC 4. Chest X-Ray:
a. Baseline
5. ECGb. Every 5 years 6. Pulmonary Function: Ratio of FEV1/FVC must be greater than 0.70 if both FEV1 and FVC are below normal 7. Urinalysis (dipstick) 8. Visual Acuity: Far (Snellen) at least 20/40 binocular corrected and at least 20/100 binocular uncorrected for those routinely using corrective lenses. 9. Color Perception 10. Stress test if clinically indicated by history or symptoms 11. Mammography: annually age 40 and older 12. Discretionary Tests:
a. TB Screen b. Hepatitis C screen c. Immunizations offered:
(i) Hepatitis B Vaccine
d. HIV screen(ii) Tetanus/diphtheria (Td) Vaccine (iii) MMR Vaccine (iv) Polio Vaccine (v) Varicella Vaccine (vi) Influenza Vaccine e. Depth perception f. Gross visual fields |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on any condition that may cause any sudden incapacitation or inability to perform duties, tendencies to seizures, dizziness, claustrophobia, loss of physical control, or similar undesirable conditions 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Written Opinion |
Job Certification with: a. Statement that the employee has sufficient strength, endurance, and emotional stability to perform the work b. An opinion the employee would not be a hazard to self or others c. Any limitations in job functions or ability to wear PPE |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| H. Food Handler | |
|---|---|
| Reference | 21 CFR § 10.115; 29 CFR § 1910.141(h) |
| Frequency |
1. Baseline Examination 2. Annual Examination |
| Laboratory |
1. TB Screening, baseline, then discretionary 2. Hepatitis A (Center may offer) 3. Discretionary Tests:
a. CBC
b. Chest X-Ray |
| Physical Exam |
1. Medical and Occupational History focusing upon transmittable infectious diseases 2. Focused Physical Examination 3. Examiner should provide counseling regarding hygiene and prevention of cross contamination/fecal-oral diseases |
| Written Opinion | Job Certification with statement that employee is medically cleared as indicated in the Food Safety section of this document. |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| NOTE: | For Crew Food Handler, refer to Primary Crew Contact Physical |
| I. Locomotive Engineer | |
|---|---|
| Reference | 49 CFR § 240.121 and Appendix F |
| Frequency |
1. Baseline Examination 2. Triennial Examination |
| Laboratory |
1. Audiogram: Hearing loss in better ear < 40 dB at 500, 1,000, 2,000 Hz with or without hearing aid 2. Visual Acuity: 20/40 with or without corrective lenses 3. Visual Fields: at least 70 degrees in each eye 4. Color: Recognize and distinguish between the colors of railroad signals |
| Physical Exam |
1. Medical and Occupational History 2. Focused Physical Examination with focus on assessing any condition affecting vision and/or hearing that may cause any sudden incapacitation or inability to perform duties, tendencies to seizures, loss of physical control, or similar undesirable conditions |
| Written Opinion | Job Certification with any limitations |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
|
J. Motive (Heavy) Equipment Operator NOTE: includes specialized maintenance and construction equipment such as bulldozers, dump trucks, etc. |
|
|---|---|
| Reference | 49 CFR subpt. E |
| Frequency |
1. Pre-placement/Baseline Examination 2. Biennial Exam 3. If Commercial Driver License required, refer to DOT/CDL |
| Laboratory |
1. Audiogram: Hearing threshold average in better ear < 40 dB (500, 1000, 2000 Hz) 2. ECG-baseline, and clinically indicated 3. Visual Acuity: 20/40 with or without corrective lenses 4. Gross Visual Fields: 70 degrees in each eye 5. Color: Recognize and distinguish between the colors 6. Urinalysis (dipstick) 7. Discretionary Tests:
a. Chest X-Ray
b. Pulmonary Function c. Blood Chemistry Profile d. Complete Blood Count (CBC) e. HbA1C (discretionary) |
| Physical Exam |
1. Occupational and Medical History 2. Physical Examination with focus on assessing any condition affecting vision and/or hearing that may cause any sudden incapacitation or inability to perform duties, tendencies to seizures, loss of physical control, or similar undesirable conditions |
| Written Opinion |
Job Certification with any limitations or referral for additional specialized clinical evaluation or testing
If an employee has Insulin Treated Diabetes Mellitus (ITDM) a FMCSA-compliant waiver is required to obtain a 12-month certification. Each Center with drivers requiring Department of Transportation (DOT) certification will have a Certified Medical Examiner. The Center's Certified Medical Examiner, civil service or contractor (per the contractor's contract) will review 1. The FMCSA ITDM Assessment Form MCSA-5870 from the employee's treating physician, per 49 CFR pt. 46. 2. A letter from employee's supervisor stating. a. The workplace is able to meet requirements to accommodate the employee such as mitigating hypoglycemic symptoms, monitoring glucose levels, and training the employee to recognize hypoglycemic episodes. b. If the heavy equipment has a dead-man switch. OCHMO will issue certifications for Centers without a Certified Medical Examiner. Occupational health clinic physicians at Centers without a Certified Medical Examiner will submit the information requested in paragraphs 1 and 2 above, along with a waiver recommendation to OCHMO within 30 days of receipt of the required FMCSA ITDM Assessment Form. |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| K. Occupational Respirator Use | |
|---|---|
| Reference | OHSA 29 CFR § 1910.134, and 29 CFR § 1910.134 Appendices A, B1, B2 , C |
| Frequency |
1. Baseline Examination 2. Baseline and annual respirator questionnaire 3. Variable or Exposure-Determined Examination |
| Laboratory | 1. Discretionary |
| Physical Exam |
1. OSHA Respirator Medical Evaluation Questionnaire (Mandatory: 29 CFR § 1910.134 Appendix A) annually 2. Focused Physical Examination with a focus on employee's ability to use a respirator for baseline 3. Annual Focused Physical Examinations required only if positive responses to Questions 1-8, Section 2, Part A of Appendix C, or at the discretion of the physician 4. Discretionary Tests:
a. Chest X-ray
b. Pulmonary Function (spirometry) |
| Written Opinion |
Required Standard Written Medical Opinion including:
a. Statement employee is medically able to use the respirator, or any limitations on respirator use related to a medical condition or related to workplace conditions in which respirator will be used
b. The need for any medical follow-up c. A statement that employee has been given a copy of the written opinion d. If the respirator is a negative pressure respirator and the PLHCP finds a medical condition that may place the employee's health at increased risk if the respirator is used, the employer shall provide a PAPR if the medical evaluation finds that the employee can use such a respirator; if a subsequent medical evaluation finds that the employee is medically able to use a negative pressure respirator, then the employer is no longer required to provide a PAPR |
| Employee Counseling | Counseling on exam results, conditions of increased risk and copy of written opinion provided to employer. |
| Medical Removal | No requirement in standard |
| L. Ordnance Handler | |
|---|---|
| Reference | |
| Frequency |
1. Baseline Examination 2. Every 2 years |
| Laboratory |
1. Audiogram 2. Visual Acuity 3. Depth Perception 4. Color Perception (as related to specific job requirements) 5. Urinalysis (dipstick) 6. Discretionary Tests:
a. ECG
e. Pulmonary Functionb. Complete Blood Count (CBC) c. Blood Chemistry Profile d. Chest X-ray |
| Physical Exam | 1. Medical and Occupational History to ascertain any condition that may cause
any sudden incapacitation or inability to perform duties, tendencies to seizures, dizziness, claustrophobia, loss of physical control, or similar undesirable conditions 2. Physical Examination focusing on strength, endurance, agility, coordination, adequate visual acuity and hearing, and emotional stability |
| Written Opinion | Job Certification with any limitations |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
|
M. Primary Animal Contact NOTE: May have to be modified to cover the animal species and specific agents being used. |
|
|---|---|
| Reference | |
| Frequency |
1. Baseline Examination 2. Annual Examination 3. Variable or Exposure-Determined Examination |
| Laboratory |
Baseline only: 1. Complete Blood Count (CBC) 2. Blood Chemistry Profile 3. Pulmonary Function 4. TB Screening 5. Tetanus every 10 years 6. Discretionary:
a. Serum Sample (10 mL) for storage
b. Rabies Titer c. Rubeola Titer d. Hepatitis A and B e. Offer Rabies Vaccine |
| Physical Exam |
1. Medical and Occupational History (annual interim history) 2. Physical Examination with focus on immunization history, conditions with suppression of the immune system, allergies to animals, and prior illnesses from animal 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use |
| Written Opinion | Job Certification with any limitations |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| N. Primary Crew Contact | |
|---|---|
| Reference | Flight Crew Health Stabilization Program JSC 22538 |
| Frequency |
1. Mission specific: No earlier than L-21 every scheduled manned launch 2. Permanent Primary Contacts: Annual 3. Food Depot: Every 6 months |
| Laboratory |
Required for Food Depot only:
(a) CBC
Discretionary Tests for all others:(b) Urinalysis (c) Blood Chemistry Panel and Cholesterol Panel (d) TB screening (annual) (e) Hepatitis A and Influenza Vaccine (offered)
(f) WBC count with differential
(g) Urinalysis (h) Other serological or bacteriological testing (i) TB screening |
| Physical Exam | Focused Physical Examination with focus on detection of infectious disease |
| Written Opinion | Certification status (JSC Form 270, KSC Form 13-116) |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| O. Security | |
|---|---|
| Reference | |
| Frequency |
1. Baseline Examination 2. Annual Examination |
| Laboratory |
1. Audiogram 2. Visual Acuity, Color Vision, Visual Field 3. ECG 4. Urinalysis (dipstick) 5. TB Screening 6. Discretionary Tests:
a. Pulmonary Function
b. Exercise Stress Test |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on ability to perform the essential functions of the job and maintain emotional stability |
| Written Opinion |
Required: a. Certification statement that the employee has emotional stability to perform the work b. In the opinion of the examiner that no medical condition was detected which would place the employee at increased risk of material impairment of the employee's health or would be a hazard to self or others c. Any limitations in job functions |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| P. Self-Contained Atmospheric Protective Ensemble (SCAPE) | |
|---|---|
| Reference | 29 CFR § 1910.134 |
| Frequency |
1. Baseline Examination 2. Annual Examination |
| Laboratory |
1. Blood Chemistry Profile 2. Complete Blood count (CBC) 3. Baseline Chest X-ray 4. Pulmonary Function 5. Audiogram: Hearing threshold ≤ 40 dB average hearing loss at 500, 1000, 2000, and 3000 Hz in the "Better Ear" 6. Visual Acuity: a. Far (Snellen) at least 20/70 in one eye and 20/100 in the other eye corrected to 20/20 in one eye and 20/40 in the other eye b. Near vision correctable to 20/40 (Snellen equivalent) bilaterally 7. Color perception 8. Depth perception 9. Gross visual fields intact 10. Discretionary Tests:
a. Annual Chest X-ray
b Urinalysis with microscopic c. ECG |
| Physical Exam |
1. OSHA Respirator Medical Evaluation Questionnaire (Mandatory: 29 CFR § 1910.134, Appendix A) 2. Physical Examination with focus on employee's ability to use a respirator under the conditions of use (i.e., temperature extremes) 3. Have sufficient strength, endurance, agility, coordination, and emotional stability to avoid interference with performance |
| Written Opinion |
Required: a. Statement that the employee is medically able to use the Self-Contained Atmospheric Protective Ensemble (SCAPE), or any limitations on SCAPE use related to a medical condition or related to workplace conditions in which the SCAPE will be used b. Any need for medical follow-up c. Statement that employer/employee has been given a copy of the written opinion |
| Employee Counseling | Counseling on exam results, conditions of increased risk and copy of written opinion provided to employer. |
| Medical Removal | No requirement in standard |
| Q. Soldering | |
|---|---|
| Reference |
IPC J-STD-001ES, Space Applications Electronic Hardware Addendum to JPC J-STD-001E |
| Frequency |
1. Baseline Examination 2. Biennial 3. Variable or Exposure-Determined |
| Laboratory |
1. Pulmonary Function (Baseline only) 2. Visual Acuity, and Color Discrimination |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination with focus on skin and respiratory tract. 3. Evaluation of ability to wear respirator may be required, see protocol Section 3 K, Certification Examination. Occupational Respirator Use 4. Evaluation of other potential exposures, e.g. lead |
| Target Organs | Respiratory, skin, varies with type of solder used |
| Written Opinion | |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| R. Voluntary Respirator Use | |
|---|---|
| Reference | OSHA 29 CFR § 1910.134 Appendix A ,B1, B2, C, D |
| Frequency | 1. Baseline Examination |
| Physical Exam |
1. Focused physical evaluation 2. History to ascertain any condition that may cause any sudden incapacitation, inability to perform duties. 3. Evaluation of ability to wear respirator under expected use conditions (i.e., temperature extremes). 4. OSHA Respirator Medical Evaluation Questionnaire (Mandatory: 29 CFR § 1910.134 Appendix A) |
| Written Opinion |
Required: a. Any limitations in job functions or ability to wear PPE |
| Employee Counseling | Counseling on exam results and conditions of increased risk. |
| A. Pilots, Flight Engineers, Other Primary Aircrew, Qualified Non-Crewmember, Unmanned Aircraft System (UAS) Pilots and Observers |
|---|
| NOTE: Refer to Section 2.2 of OCHMO 110902MED; NPR 7900.3 Aircraft Operation Management Manual; 14 CFR pt. 67 Medical Standards and Certification for certification examination requirements. |
| B. Air Traffic Control Specialist (Not requiring FAA Certification) | |
|---|---|
| Reference | Office of Personnel Management (OPM) GS-2152 |
| Frequency |
1. Baseline Examination 2. Annual Examination |
| Laboratory |
1. Audiogram: No hearing loss in either ear of more than 25 decibels at 500, 1000, or 2000 Hz. No hearing loss in these ranges of more than 20 decibels in the better ear. 2. Visual Acuity:
a. Distant 20/20 in at least one eye with or without correction
3. Visual Fields: Normalb. Near vision 20/20, Snellen equivalent, with or without correction 4. Color Vision 5. Tonometry 6. ECG 7. 8. 9. Discretionary Tests:
a. Blood Chemistry (can include fasting blood sugar and blood lipid profile).
b. Complete Blood Count (CBC) c. Chest X-ray d. Pulmonary Functions e. Urinalysis (dipstick) f. Exercise Stress Test |
| Physical Exam |
1. Medical and Occupational History 2. Physical Examination (see OPM qualifications on age based blood pressure values) with focus on cardiovascular, neurological, musculoskeletal, general medical, psychiatric, and substance dependency |
| Written Opinion | Certification with any limitations |
| C. Second Class Airman's Medical Certificate (Air Traffic Control Tower Operator) | |
|---|---|
| Reference | 14 CFR pt. 67 Appendix A |
| Frequency |
1. Baseline Examination 2. Annual Examination |
| Laboratory |
1. Audiogram See FAA II 2. Visual Testing and Requirements: See FAA II 3. ECG (transmitted to FAA): First examination after 35 years of age, and annually after 40 years of age 4. Discretionary Tests:
a. Blood Chemistry Profile (can include fasting blood sugar and blood lipid profile)
b. Complete Blood Count (CBC) c. Chest X-ray d. Pulmonary Function e. Urinalysis (dipstick) f. Exercise Stress Test |
| Physical Exam |
1. Medical and Occupational History
2. Physical Examination by FAA certified physician with
focus on any condition that may cause any sudden
incapacitation or inability to perform duties, tendencies
to seizures, dizziness, claustrophobia, loss of physical
control, or similar undesirable conditions 3. Average BP should not exceed 155mm/95mm 4. Check references above for acceptable standards, equipment, and requirements. |
| Written Opinion |
a. Certification with any limitations, or referral to Aerospace
Medical Certification Division, or Regional Flight Surgeon
for possible further specialized clinical evaluation or
testing. b. See 14 CFR pt. 67 for Pilot Medical Standards |
| A. Fitness For Duty (FFD) | |
|---|---|
| Regulation | |
| Defined | Fitness for Duty (FFD) examinations are performed at the request of management when a change in work performance, productivity, or health is observed or suspected. |
| Frequency | Variable upon an unexpected change in behavior or performance. The examination should be completed as soon as possible after a written request through management has been made |
| Scope | The physician should evaluate whether there is a medical or psychological condition impacting work performance. A job description with the physical requirements and essential job functions is an integral part of this evaluation. Cooperation and coordination with the treating physician(s), as well as other services such as the Employee Assistance Program (EAP) can be of help to an affected employee |
| Managers Responsibilities |
The supervisor/manager requesting the FFD examination should notify the employee and have their consent, provide documentation to the physician and a copy of the employee's job description.
Managers must also decide if there is a "For Cause" need for drug testing based upon performance. Since this testing is not a medical test, the manager must contact the Drug Free Workplace (DFW) coordinator to arrange testing |
| Laboratory | Discretionary |
| Confidentiality | Confidentiality is of utmost importance and all recommendations and reports must be limited to work-related matters, e.g., work limitation, modifications, or accommodations. No non-work related medical diagnosis should be released in the written opinion |
| Written Opinion | Required return to duty status for the employee's manager, including recommendations for work limitations or accommodations |
| B. Return to Work (RTW) | |
|---|---|
| Regulation | |
| Defined | RTW evaluations are usually performed when employees are returning to work after an illness or injury of greater than 3 business days |
| Frequency | Variable or Exposure-Determined Examination |
| Scope |
1. Vital signs 2. The evaluation should focus on the employee's ability to perform the essential job functions with or without work limitations, modifications, or accommodations. The information from the employee's physician is reviewed, and a decision is made whether a focused physical and/or tests are necessary |
| Managers Responsibilities | The manager requesting the RTW examination must provide a copy of the employee's job description that includes the functional and physical requirements |
| Laboratory | Focused laboratory based upon the prior condition/problem of the employee |
| Confidentiality | Confidentiality is of utmost importance and all recommendations and reports must be limited to work-related matters, e.g., work limitation, modifications, or accommodations |
| Written Opinion |
A RTW certificate for the employee's manager should indicate: a. A statement of work limitations (including modifications and duration) b. A statement of any Personal Protective Equipment (PPE) needed or limitations in use of PPE c. For an occupational related issue, safety, and health should receive a copy of the RTW statement |
| C. International Traveler | |
|---|---|
| Reference | CDC |
| Frequency |
1. Variable or Exposure-Determined Examination 2. NOTE: Medical clearance required for NASA civil service employees traveling outside the United States or its possessions, with special emphasis for those traveling to Russia or the former nations under the Soviet Union, TAL site, or any developing or medically under-served country |
| Laboratory | Immunizations offered based on recommended WHO and CDC country requirements |
| Physical Evaluation |
1. Medical Record Review 2. Medical and Occupational History 3. Physical Examination (discretionary) 4. Offer HRA 5. Provide education based on health risk assessment with emphasis on food and water precautions and other specific issues related to travel destination |
| Written Opinion (Clearance) | As required by Center policy |
| A. Preventive Health Examination | |
|---|---|
| Reference | U.S. Preventive Services Task Force |
| Frequency |
1. Offer annually to NASA employees 2. Offer at retirement to NASA employees if not previously done |
| Laboratory |
1. Vital signs 2. Total body skin examination: baseline and at providers discretion 3. BMI 4. Baseline and at providers discretion: a. Visual Acuity b. Audiogram c. Pulmonary Function d. ECG 5. Breast examination 6. PAP smear (at clinical discretion) 7. PSA test (at clinical discretion) 8. Digital Rectal examination offered to men age 40 and older 9. Complete Blood Count (CBC) 10. Blood Chemistry Profile (includes fasting blood glucose) 11. Lipid profile 12. Urinalysis 13. High Sensitivity Fecal Occult Blood |
| Physical Exam |
1. Medical and Family History, if history of smoking -- offer smoking cessation 2. Physical Examination Complete baseline then focused as clinically indicated |
| Counseling/ Education |
1. Tobacco cessation, if indicated 2. Healthful diet and physical activity 3. Risk factors based on age, history and examination 3. Breast or testicular self-examination 4. Mammograms every 1-2 years age 40 to 49, every 2 years for age 50 to 74 5. Colonoscopy every 10 years after age 50, earlier with family history (refer to private MD) |
| Target Organs | Multiple Organs |
| Written Opinion | A summary of examination and laboratory results provided to the employee along with individualized preventive health recommendations |
| B. Fitness Center Clearance | |
|---|---|
| Reference | |
| Frequency | Per Center or component facility policy |
| Laboratory | Discretionary |
| Physical Exam |
1. Review of Physical Activity Readiness Questionnaire (PARQ), if applicable 2. Vital signs (blood pressure, pulse) 3. Physical examination and testing as clinically indicated. Refer to primary care provider as appropriate for additional testing/documentation. Medical Director must review documentation provided by primary care provider. |
| Written Opinion (Clearance) | Medical clearance may specify any limitations in clearance duration (i.e., 1-year) or Fitness Center activity |